Asia-Pacific Chiropractic Journal
Issue 7-1 Published 1 July 2026;
Next issue: 1 Sept 2026
Anywhere, anytime, any language, in your pocket
Select language here
Editorials
AU: Phillip Ebrall, BAppSc(Chiropr), GC Tert Learn Teach, MPhotog, PhD, DC (Hon), FACCS, FICCS. Director, Chiropractic Education and Research, Chiropractic India. pebrall@me.com
Narrative: Concern is expressed over the flippant language used to describe the discipline of Chiropractic as used by the inaugural head of a new program of Chiropractic education in Australia.
The program launched at Victoria University in 2026 with an initial cohort of 8 students for the year. This contrasts to the usual intake of the prior program, at RMIT University of some 60 to 80 commencing students annually.
Appreciation is given to the Australian Chiropractic College, originally founded in Adelaide, for now opening a handsome campus in the prime Melbourne legal district and which is attracting strong interest.
Indexing Terms: Chiropractic; education; social media; Australia.
Cite: Ebrall P. ‘Do you strike a pose or make a difference’. Asia-Pac Chiropr J. 2026;7.1. https://www.apcj.site/EditorialEbrallJuly26.pdf
Take-away: '… there is nothing sadder than a Baby Boomer trying to appear trendy on social media for aspirational millennials about to invest $150,000 in their future as a Chiropractor …’
Introduction
Taking full responsibility for competently teaching future Chiropractic professionals is a serious, high-impact commitment, especially given the discipline’s ongoing evolution, evidence base debates, and the imperative to produce safe, competent, ethical practitioners who can thrive in the 21st Century modern healthcare environment in any country. I am not sure the inaugural head of the Chiropractic program at Victoria University, Melbourne Australia, understands this.
Victoria University and Chiropractic
Kenneth J Young’s body of scholarship (1, 2) shows he adds little that is helpful to the discipline, rather he parrots the manifesto of Walker’s ‘New Chiropractic’ (3) which failed to land at the University of Lancashire (UCLan). (4) That program was announced mid 2019 (5) and Young became the Lead (designate) for Chiropractic at UCLan 6 months later, in December 2019. The University terminated the implementation of the program about a year later, February 2021. Young’s substantive appointment was as a Senior Research Fellow in Musculoskeletal Health, and his appointment to VU was announced in January 2025. It must be said that there is nothing censorious about leading a failed implementation, these things happen in higher education and there are always lessons to be learned.
It did not help that the number of students in Chiropractic programs in the UK were documented in June 2024 (6) as falling by n = 75 students (5%) to just 1,583 total for approved programmes across all the years, an average of 316 students per program over 5 programs. It also did not help that UCLan opened a medical program in 2015, (7) a known source of political resistance for Chiropractic education.
Of course, UCLan cited the ongoing pandemic situation and associated financial restraints as the reasons for dropping the Chiropractic program. Young remained optimistic, saying ‘The possibility of taking it up again in future years has not been ruled out and, as the course was approved last September, we have a viable curriculum that could be implemented with minimal effort, should conditions prove more favourable at another time’. (4) He ‘transferred over’ to the research team to keep working on the projects he initiated since the deferral of the course and then departed the UK to return to Australia.
Given the forgoing it is to be expected that his implementation of a program of Chiropractic education at Victoria University in Melbourne Australia is drawing more than the usual interest from the profession. Judgement is delayed in the absence of a publicly available curriculum. It is unfair to deduce what is being taught from some abbreviated course outlines. I could not locate a statement of the philosophical stance the program will take, nor a statement of the program’s Educational Philosophy. There is, however, a reliance on the dated trope of ‘evidence based practice’. All that the University’s News Centre provided the Journal is a press release and a couple of images. one of which we reproduce here.
We are left with vacuous on-line words suggesting the program will be evidence-based, Walker’s mantra for his New Chiropractic, and the untested hope that students will absorb the essence and bonhomie of Chiropractic in just 4 weeks a semester. This reflects VU’s novel idea that ‘block teaching’, where one course is delivered in full over one 4-week block in a semester, will actually produce graduates with a strong professional identity, as opposed to merely ticking boxes of academic attainment. We note that VU’s review (8) after 5 years of implementation shows ‘Increases in student success measures’ and ‘equity group students in first year units reported higher pass rates, closing the gap to non-equity group students’, both valuable educational outcomes. We also note a number of other scholarly papers which are favourable to the concept for its improvements in student performance and retention.
What is not known of course is whether periodic engagement in a discipline will be effective as opposed to immersion over a full 16-week semester. I suspect there may be challenges here given that in their first year at VU, Chiropractic students receive only 4 calendar weeks per semester of ‘Chiropractic’ to instil professional behaviours and an understanding of the philosophical positions within the discipline. I am uncomfortable with this experiment.
In terms of the contemporary understanding of philosophical positions in Chiropractic, (9) Young is one of the discipline’s minority post-realists yet he beat out at least one other highly competent applicant, a conventional realist representing the majority. The Journal questions whether Walker was a member of the VU selection committee for the position to which Young was the successful applicant. I ask on the basis that Walker was Young’s supervisor for his PhD, a matter which in the real world of ethics and professional behaviour outside the shelter of Australian universities would have demanded Walker recuse himself from selecting his protégé for appointment to the position. I would like to believe he did.
Regardless, whatever has happened has happened. It is not helped by Young’s inane attempts on social media to be seen as a trendy Gen Z communicator; it is sad to see a Baby Boomer making a fool of himself in this manner. It could be argued by formal notification to AHPRA that public videos of this nature bring the profession into disrepute. It is a matter of record that Australian Chiropractors have been reprimanded for less egregious positions on social media.
I noted earlier that UCLan terminated the implementation of its Chiropractic program in February 2021, very soon after announcing it and appointing Young as foundation head. It would not surprise me for VU to do the same and also rid itself of these embarrassing, puerile clips. They really must be taken down immediately.
After all, 8 students in the initial cohort is not financially sustainable. Vice-Chancellor Shoemaker seems to know a little about Chiropractic yet can not be presumed to have any duty of care to the discipline. He will be driven by the numbers, and the numbers tell me as an academic with experience in these matters, that the VU program has also failed to land. Just how costly a failure it becomes depends on when the University bites the bullet, kills it, and transfers its 8 students.
Conclusion
Peta Credlin, Australian political commentator, is acknowledged for her quote used as the title of this piece. It seems to me that the Walker-driven ‘New Chiropractic’ program being introduced by Ken Young at Victoria University Melbourne is simply striking a pose. It is a pose of the ‘evidence-based movement’ discredited in 2006 by Holmes et al (10) and largely rejected by medicine. (11, 12) The real issue not being addressed is the ‘Evidence-Practice Gap’. (13)
In stark contrast, the ‘chiropracticness’ (14) of the open evening at the Melbourne Campus (Figure 2, below) of the Australian Chiropractic College in May 2026, which I attended at my own expense (meaning I was not a paid guest and thus have no obligations to discharge), was joyous and wonderful.
In his welcoming address the President of ACC, Dr Pat Sim, spoke to the purpose of being a Chiropractor. The contrast with Ken Young not knowing why he’d ‘crack’ a neck was stark and revealing. Figure 3, below, shows a class of ACC students settling into their new campus.
Young seems to lack a reasonable sense of professional identity. He may well be adored within Chiropractic Australia, but this minority group of dissidents has no substantive meaning in Australia’s bigger picture.
For me, a program of Chiropractic education must achieve two things:
- a graduate who is a compassionate, well-informed doctor who applies best available evidence to provide optimal care with intent for the patient at that time, and
- a graduate with a strong professional identity as a Chiropractor. The published, indexed evidence (15-18) is that a strong professional identity is the hallmark of a strong profession globally.
There is no doubt in my mind that my recommendation to emerging Chiropractors is to attend the Australian Chiropractic College, either the Melbourne or the Adelaide campus. At the very least you will learn how to adjust the cervical spine, with intent.
As a final note of dismay for the future of Chiropractic in Australasia, it has been announced (19, 20) that Young was appointed to the Chiropractic Board of Australia. It is at this point that one gives up all hope of people being appointed on merit instead of through an old mate’s network.
References
- Young KJ. Gimme that old time religion: the influence of the healthcare belief system of chiropractic's early leaders on the development of x-ray imaging in the profession. Chiropr Man Therap. 2014;22, 36. At https://link.springer.com/article/10.1186/s12998-014-0036-5#citeas
- Kerry R, Young KJ, Evans DW et al. A modern way to teach and practice manual therapy. Chiropr Man Therap. 2024;32,17. At https://link.springer.com/article/10.1186/s12998-024-00537-0#citeas
- Walker BF. The new chiropractic. Chiropr Man Ther. 2016;26(26). At https://link.springer.com/article/10.1186/s12998-016-0108-9
- Society for promoting Chiropractic education. University of Central Lancashire (UCLan) course not be proceeding. News. 26 February 2021. At https://chiroeducation.org/news/university-central-lancashire-uclan-course-not-proceeding/
- World Federation of Chiropractic - WFC. Facebook post. 24 June. 2019. At https://www.facebook.com/WorldFederationofChiropractic/posts/new-uk-chiropractic-program-announced-the-uks-university-of-central-lancashire-u/2157292634392974/
- Overview of Chiropractic Education. GCC Annual Report. June 2024. At https://www.gcc-uk.org/assets/publications/2024_overview_of_chiropractic_education.pdf
- University of Central Lancashire. Medical School. The Medic Portal. n.d. At https://www.themedicportal.com/school/university-of-central-lancashire/
- Evaluating VU Block Model 5 years on. VU Block Model Equity Cohort Analysis Extract. Victoria University. 2023. At https://www.education.gov.au/system/files/2023-09/AUA_inter_tranche15_207%20Victoria%20University%20Attachment.pdf
- Ebrall P. Changing chiropractic’s subluxation rhetoric: Moving on from deniers and vitalists to realists, post-realists, and absurdists. Asia-Pac Chiropr J. 2022;3.3. https://www.apcj.net/Papers-Issue-3-3/#EbrallRhetoric
- Holmes D, Murray SJ, Perron A, et al. Deconstructing the evidence-based discourse in health sciences: truth, power and fascism. International Journal of Evidence-Based Healthcare. 2006;4:180-6. At https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1479-6988.2006.00041.x
- Miller C, Miller D. The Real World Failure of Evidence-Based Medicine. Int J Person Centered Med. 2011;1(2):295-300. At https://www.researchgate.net/publication/233412662_The_Real_World_Failure_of_Evidence-Based_Medicine#fullTextFileContent
- Venus C, Jamrozik E. (2020), Evidence-poor medicine: just how evidence-based are Australian clinical practice guidelines?. Intern Med J. 2020;50:30-7. At https://onlinelibrary.wiley.com/doi/full/10.1111/imj.14466
- Kim SY. Evidence-based practice and evidence-practice gap: status, challenges, and solutions. J Evid-Based Pract. 2025;1(1):1-6. At https://www.e-jebp.org/journal/view.php?number=4
- Charlton KH. A Chiropracticness Test. Chiropr Osteopat. 2005 Nov 24;13:24. DOI 10.1186/1746-1340-13-24.
- Glucina T, Gaskin H, Fox M, Holt K. Practice characteristics of New Zealand chiropractors: A 2019 survey. Asia-Pacific Chiropr J. 2021;1.3. https://www.apcj.net/glucina-et-al-demographics-new-zealand/
- Richards D, Grace S. Statistical analysis of the results of a survey on the meaning and value of Vitalism in Chiropractic. J Contemp Chiropr. 2026;9(1):142-57. At https://journal.parker.edu/article/158796-statistical-analysis-of-the-results-of-a-survey-on-the-meaning-and-value-of-vitalism-in-chiropractic
- Naidoo S, Mitchell SL, Paton GJ. Chiropractic identity, role, and future: A secondary analysis of a survey of South African chiropractors. J Chiropr Humanit. 2025;32:16-24. At https://www.sciencedirect.com/science/article/pii/S1556349925000026
- Ebrall P. Finding the professional identity of chiropractic in Australasia that shaped education: A pragmatic narrative of the Inquiry Period from 1960 to 1979. Asia-Pac Chiropr J. 2022;3.1. https://www.apcj.net/papers-issue-3-1/#InquiryPeriod
- Dr Kenneth Young joins the Board. Chiropractic Board of Australian. Newsletter. May 2026. At https://www.chiropracticboard.gov.au/News/Newsletters/May-2026.aspx#Kenneth-Young
- Dr Kenneth Young joins the Chiropractic Board of Australia. Chiropractic Australia. Wednesday 20, May 2026. At https://www.chiropracticaustralia.org.au/news-item/23380/dr-kenneth-young-joins-the-chiropractic-board-of-australia
AU: Charles S Masarsky DC. Private practice of Chiropractic, Vienna VA. e: viennachiropractic@verizon.net
Narrative: Even today I meet Chiropractors with only a vague idea of their professional identity. For me, my identity as a Doctor of Chiropractic was forged at Palmer College from the words of the discipline’s founder, DD Palmer, and one of its greatest educators, AE (Earl) Homewood. I was clear in my mind about Chiropractic's Grand Strategy.
Here I propose that readers contribute to a refreshed Chiropractic Grand Strategy, one that is clear about our purpose and why we do what we do, daily in practice to improve the health and well-being of our patients.
I see value in refining our Grand Strategy and propose a straight forward 50-word strategy which avoids political posturing and presents a clear position to better unite Chiropractors as a professional group.
Indexing terms: Chiropractic; professional identity; grand strategy.
Cite: Masarsky CS. Homewood, Holism, and Strategy: The wide-angle lens. Asia-Pac Chiropr J. 2026;7-1. At
Take-away: '… too many of our colleagues have only the foggiest notion of what the Chiropractic profession is trying to do in the world …’
The fog
A number of years ago, my practice partner (Dr Marion Todres-Masarsky, my wife) and I were invited to a meeting sponsored by a spinal surgery practice. The practice owners wanted to explore the possibility of research collaboration with local Doctors of Chiropractic. Needless to say, we were delighted to attend, along with some twenty other practitioners.
The sponsor’s research director passed around a list of Chiropractic research citations, stating that this was the sole result of her ‘extensive’ literature search. The list was barely a page long. No mention of the NINCDS study, the New Zealand report, the Journal of Manipulative and Physiological Therapeutics, Chiropractic Technique, the Journal of the Canadian Chiropractic Association, the Chiropractic Journal of Australia, to name a few chiropractic research publications readily available at that time. The research director’s smug certainty about our supposed paucity of evidence seemed comical, given her abysmal ignorance about chiropractic research. Disturbingly, few of our colleagues seemed to think anything was amiss.
When the discussion seemed to be going nowhere, I suggested we go around the room and state which Chiropractic technique we generally use. What I had in mind was getting a general idea of the sorts of outcome measures that could be used in this proposed collaborative setting. I assumed that this group of mostly young practitioners would be mentioning such techniques as Gonstead, NUCCA, AK, and SOT, perhaps along with some techniques that were new to me. Instead, one of them mentioned core strengthening. The next one spoke of Pilates training. I interjected, suggesting that these were excellent adjuncts to the Chiropractic adjustment, but what actual adjusting techniques do you use? The next speaker stated, ‘Sometimes I manipulate’. Most of the other attendants had a somewhat puzzled expression … directed at me!
More recently, I was presenting a continuing education seminar on the topic of Chiropractic care of long COVID victims. In general, the audience was interested and receptive. However, one of the attendees objected to the topic. He ‘reminded’ me that COVID is a viral infection, and we’re not virologists.
Experiences similar to those I just described have made it clear to many of you that too many of our colleagues have only the foggiest notion of what the Chiropractic profession is trying to do in the world. Perhaps the external pressures of economics, the insurance industry, and the medicolegal establishment have been internalised by many of our colleagues. This phenomenon of paradigm erosion was already decades old when I co-authored a paper on the topic in 1991. (Masarsky CS and Weber M, 1991)
One thing that may be helpful in ameliorating our profession’s paradigm erosion is something equivalent to what nations call ‘grand strategy’.
Grand strategy
Generally speaking, ‘grand strategy’ is an over-arching idea that informs the more specific goals and activities of a nation. Grand strategy is often discussed in military terms, but it also relates to the diplomatic, economic, educational, and cultural spheres. History records several consequential examples of national grand strategies.
For example, Pax Romana was the grand strategy of ancient Rome in the 1st century. Isolationism was the grand strategy of China from the 14th through the 17th Century, Japan from the 17th to the 19th Century, and the United States intermittently from the 18th to the 20th C. Mercantile colonialism was the grand strategy of Spain and Portugal in the 16th Century, soon to be joined by Britain and France until the 18th Century.
Health professions exist for the purpose of promoting the longevity and quality of life for those under their care. Practitioners of all schools have this general purpose in common, and it certainly should form the embryo of any health profession’s grand strategy. Strategic elements more specific to a particular profession can be based on principles drawn from such paradigms as allopathy, homeopathy, and as I hope to demonstrate, chiropractic.
Homewood’s hints towards a Grand Strategy
During my initial Chiropractic education, I was strongly influenced by Homewood’s The Neurodynamics of the Vertebral Subluxation. (Homewood AE, 1977). For me, Homewood's understanding of DD.Palmer’s concept of tone was the key insight. (Palmer DD, 1910) Certainly, disturbed spinal nerve function can disrupt musculoskeletal tone, leading to back pain, neck pain, and so forth. However, Homewood reminded us that disturbed spinal nerve function does not disrupt musculoskeletal tone only. The neurodynamics of the vertebral subluxation can influence vasomotor tone, alimentary tone, bronchial tone, and all other aspects of tone.
Clearly, the Palmer-Homewood concept is holistic. However, its holistic lens is quite distinct from that of herbal medicine, aroma therapy, and many other disciplines. The specific yet holistic concern with disturbed nerve function as it affects somatic and visceral tone has been described as neurologic holism. (Masarsky CS, Todres-Masarsky M, 2001)
Draft of a Grand Strategy
Centering a chiropractic grand strategy on neurologic holism’s approach to tone offers several advantages. It does not have to be subluxation-based or scientific; it can be subluxation-based and scientific. Its basis can be firmly anchored in well-recognised anatomical reality. A grand strategy based on neurologic holism does not have to promote a chiropractic profession that is either cooperative or independent; it can be cooperative and independent.
As a starting point, I offer the following draft of a chiropractic grand strategy:
Neurologic Holism: The chiropractic profession is concerned with improving longevity and quality of life by assessing and correcting biomechanical interference with the neurological coordination of somatic and visceral tone. This concern informs the profession’s approach to clinical assessment, clinical intervention, professional and public education, scientific research, interprofessional cooperation, and public health policy.
Let’s talk
Would a Chiropractic grand strategy be beneficial? If so, is the proposed draft moving in the right direction, or should it be something quite different? How could a grand strategy guide the specific strategic components stated above (assessment, intervention, research, etc.) in a practical sense? Please address your comments in a Letter to the Editor. I will attempt to answer all such letters thoughtfully. In this way, we can have a robust discussion of chiropractic grand strategy in this readily accessible publication.
Editor's note
In 1991 (Masarsky & Weber) the author took a confidently normative stance, arguing for a shift in both practice and research that would distinguish Chiropractic as a distinct scientific enterprise. He and Weber combined critique of the profession’s current constraints with a constructive agenda, outlining specific research directions and interdisciplinary connections (ergonomics, somatic disciplines, aging). As in this piece in 2026, Masarsky made a clear argumentative arc: diagnose the problem, illustrate with clinical vignettes, propose a reoriented research program, and envision broad, long-term implications.
The outcome is a dialogic, somewhat provocative tone that challenges mainstream medical paradigms while inviting philosophical and empirical collaboration.
Ebrall assisted by Grok
References
- Homewood AE. The Neurodynamics of the Vertebral Subluxation. Valkyrie Press, St Petersburg, Florida, 1977.
- Masarsky CS, Weber M. Stop Paradigm Erosion. J Manipulative Physiol Ther, 1991; 14: 323-326.
- Masarsky CS, Todres-Masarsky M. Neurologic Holism: Chiropractic’s Scientific Future. In: Somatovisceral Aspects of Chiropractic: An Evidence-Based Approach. Churchill Livingstone, New York, 2001.
- Palmer DD. The Science, Art, and Philosophy of Chiropractic, p 827. Portland Printing House, Portland, OR, 1910.
Dr Masarsky's YouTube channel
Dialogue

'The updated concept of functional neurology represents the neuron integrated into its environment and therefore susceptible to modulations of its signalling capacity by a vast array of external factors …’
Narrative: In this review I first identify the conditions that may be assessed using Functional Neurology and then describe the neuron and the many processes associated with neuroplasticity and neural signalling.
Then I offer a comprehensive review of the effects of modalities upon neuroplasticity and neurogenesis, giving mechanisms and signalling pathways relevant to clinical observation. I finish with a discussion on nutrients found to affect cognitive function and propose mechanisms for their effectiveness.
I conclude that the updated concept of functional neurology represents the neuron integrated into its environment and therefore susceptible to modulations of its signalling capacity by a vast array of external factors. These agents of change include both electrical and chemical phenomena triggered by such external interventions as rehabilitation, manual muscle therapy, acupuncture, biofeedback, aromatherapy, yoga, cognitive exercises, eye muscle exercises, mediation, exercise, diet, and botanical nutritional supplements.
Indexing terms: Chiropractic; functional neurology; neuroplasticity; clinical intervention; nutrients.
Cite: Rosner AL. Functional neurology: A review. Asia-Pac Chiropr J. 2026;7-1. https://www.apcj.site/RosnerFunctionalNeurology.pdf
Introduction
A discussion of the meaning and scope of functional neurology is perhaps best introduced with a quotation from the individual responsible for the origins of Chiropractic, DD Palmer:
‘Life is the expression of tone’. In that sentence is the basic principle of Chiropractic. Tone is the normal degree of nerve tension. Tone is the expression of function by normal elasticity, activity, strength, and excitability of the various organs as observed in a state of heath. Consequently, the cause of disease is any variation of tone, nerves too ‘tense’ or’ static’. (1)
Specifically, functional neurology can be thought of as a master biomarker, in that it utilises an entity that acts as the origin of changes in health that, if left unattended, emerge as symptoms and ultimately as pathologies.
That entity is the nervous system, lending itself to an assortment of noninvasive tests designed to pinpoint the area of neural dysfunction and helping to identify the optimal stimulant to activate that area, ideally before more substantial disorders appear.
Functional neurology is founded on the principle of neuroplasticity, in that nerve connections in the brain may be modified or shaped by a variety of afferents, including sensory, cognitive, emotional, or motor experiences, and thus amenable to rehabilitation. It stands in contrast to previous scientific tenets that brain development is limited to a critical period in early childhood, remaining relatively unchanged thereafter. (2)
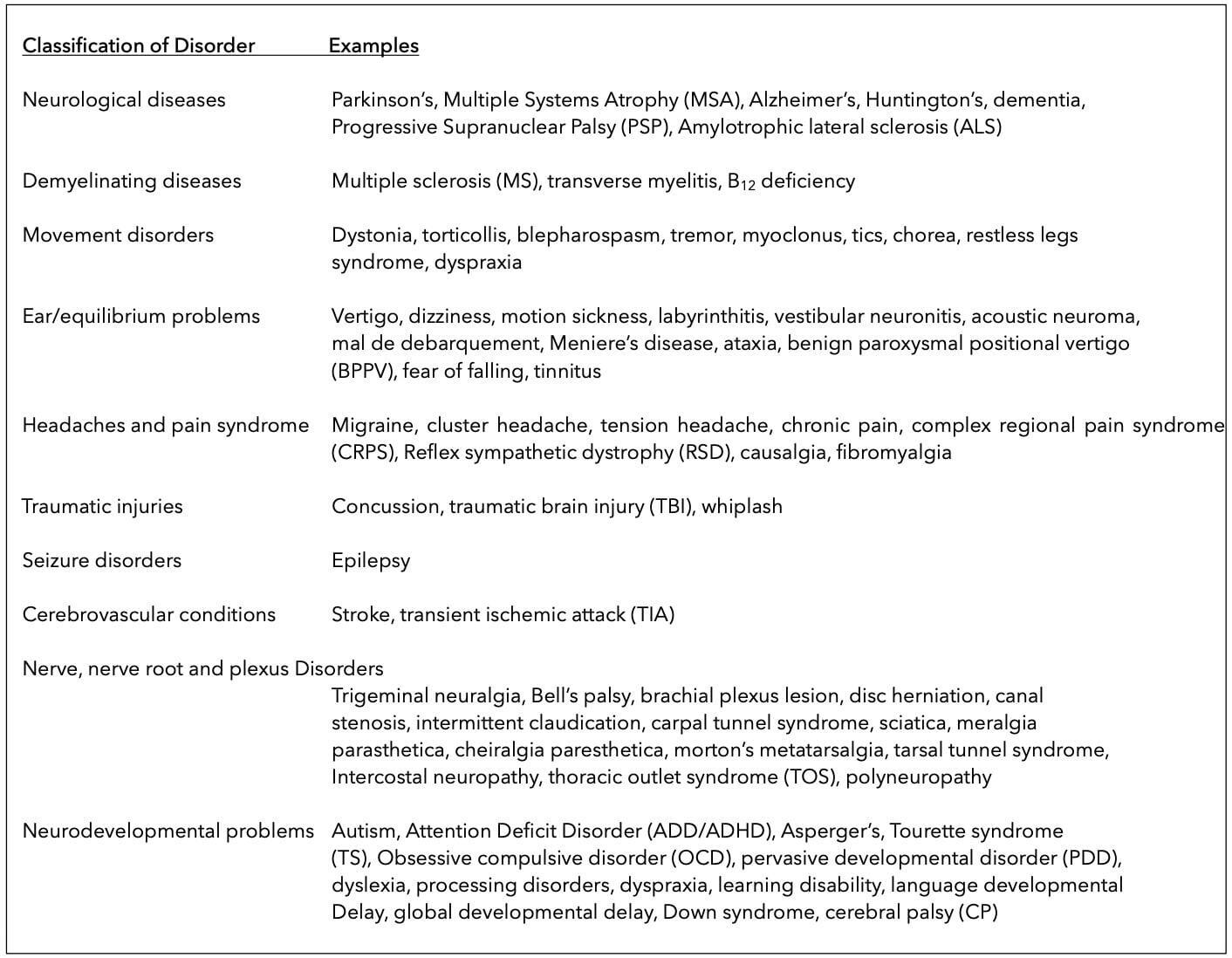
Clearly the focus of functional neurology is the conceptualisation of the nervous system as an integrated network which controls the homeostasis of the body through balanced signalling, free from distortions which could lead to a variety of conditions as suggested by Table 1. (3)
Table 1: Conditions address with Functional Neurology
The positive aspect of functional neurology is that a reorganisation of nerve cells is possible to restore or bypass the connections that have become disrupted or damaged, a perfect example being exercises to recover from stroke. The negative aspect, however, is that if a neuronal pathway is not fired, synaptic connections may become inactive with the loss or inactivation of neurotransmitters and receptors, as exemplified by the abundance of mental exercises designed to forestall cognitive decline in the elderly. (4, 5)
It can be concluded from the preceding discussion that functional neurology is an approach that is multidisciplinary, open to conceptual and therapeutic contributions from any of an extensive variety of healthcare professions, including medical doctors, doctors of osteopathy, Chiropractors, doctors of naturopathy, physical therapists, occupational therapists, doctors of optometry, doctors of oriental medicine and acupuncture, dentists, and nurse practitioners, as well as toxicologists and neuroscientists.
- The focus of functional neurology is upon strategies to promote brain function with attention to brain exercises, diet, nutrition, lifestyle, and environmental factors.
The neuron
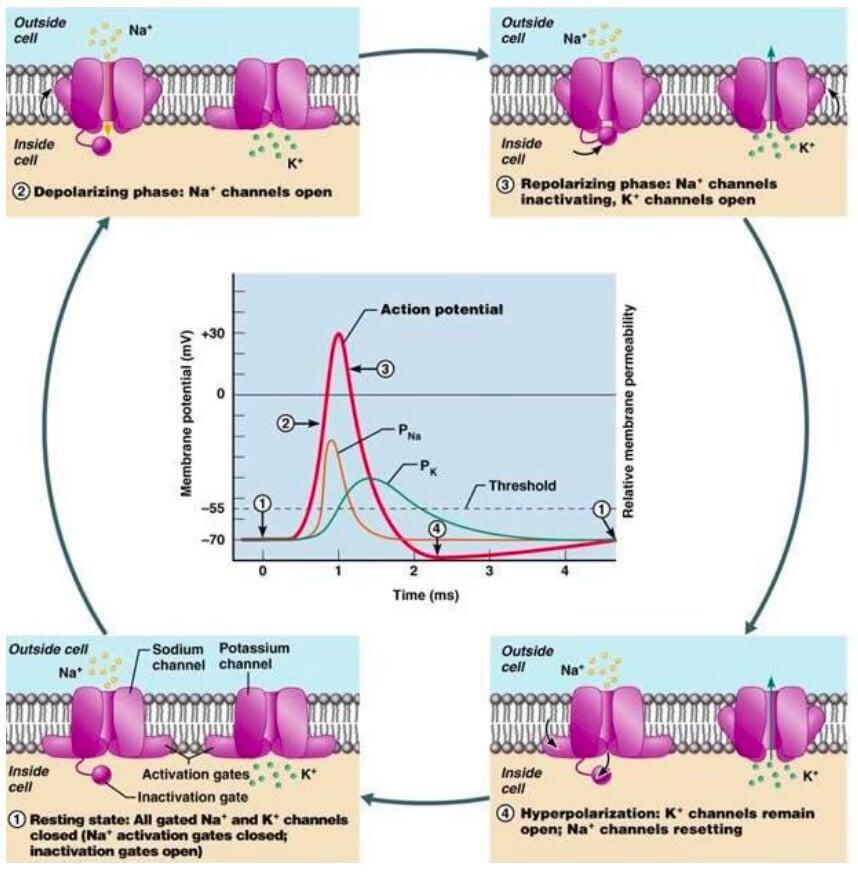
An understanding of functional neurology should begin with the neuron. (6) Here it is a matter of assessing the likelihood that the neuron will produce an action potential, depending upon its state of polarisation. This, in turn, depends upon the sum total of the excitatory and inhibitory stimuli that it encounters at any given moment. If the neuron is in a depolarised state, the cell has become more positive internally, minimising the potential difference across the membrane and thereby moving the neuron toward its firing threshold.
This may be accomplished by the movement of positive sodium ions into the cell. Conversely, hyperpolarisation occurs when the cell interior has become more negative, increasing the potential difference across the membrane and causing the neuron to back away from its firing threshold. This state may be achieved by the efflux of positive potassium ions from the cell’s interior or by the entrance of negative chloride ions into the neuron.
Calcium ions may also be involved in modulating membrane permeability and thus the firing threshold. Ion movements across the membrane are achieved through what are known as voltage gated channels. The depolarisation and hyperpolarisation cycle involving sodium and potassium ions is illustration in Figure 1. (7)
Figure 1: Firing and quiescence of the neuron: Mechanism of action via polarisation and depolarisation
Neuroplasticity
The reorganisation of nerve cells is the core concept of functional neurology; i.e., changes in the physiological function of the neuro-axis in response to changes in the immediate or external surroundings, was first identified anatomically in 1964 when the histology of the rat cerebral cortex was found to respond to environmental changes. (8) But indications of the brain’s ability to reorganise in response to the environment were reported over a century ago in the writings of Shepherd Ivory Franz, who first reported that monkeys that were subjected to mechanical stimulation of the peripheral nerves and muscles recovered from an induced paralysed condition of the arm to normal movement. (9) That same year, Franz and two coauthors reported in 5 subjects with paralysis of 5-20 years’ duration that voluntary motor control was restored with a rehabilitation program including massage, and shaking of the affected limb. (10)
Franz speculated that ‘it is apparent that some possibility of functional adaptation exists in the brain for certain types of movements so that when a certain ‘centre’ and its connected muscles cannot be utilised, other ‘centres’ and their connecting muscles may be brought into play to bring about the desired result’. (11) It was just 30 years ago, however, that the World Health Organisation acknowledged that neuroplasticity could play a role in the repair of the central nervous system and thus might be a factor in effective healthcare interventions. (12) Not long afterward, these therapeutic interventions were soon deemed to be effective in counteracting lesions of the central nervous system regardless of whether they were applied acutely, sub-acutely, or late after injury. (13)
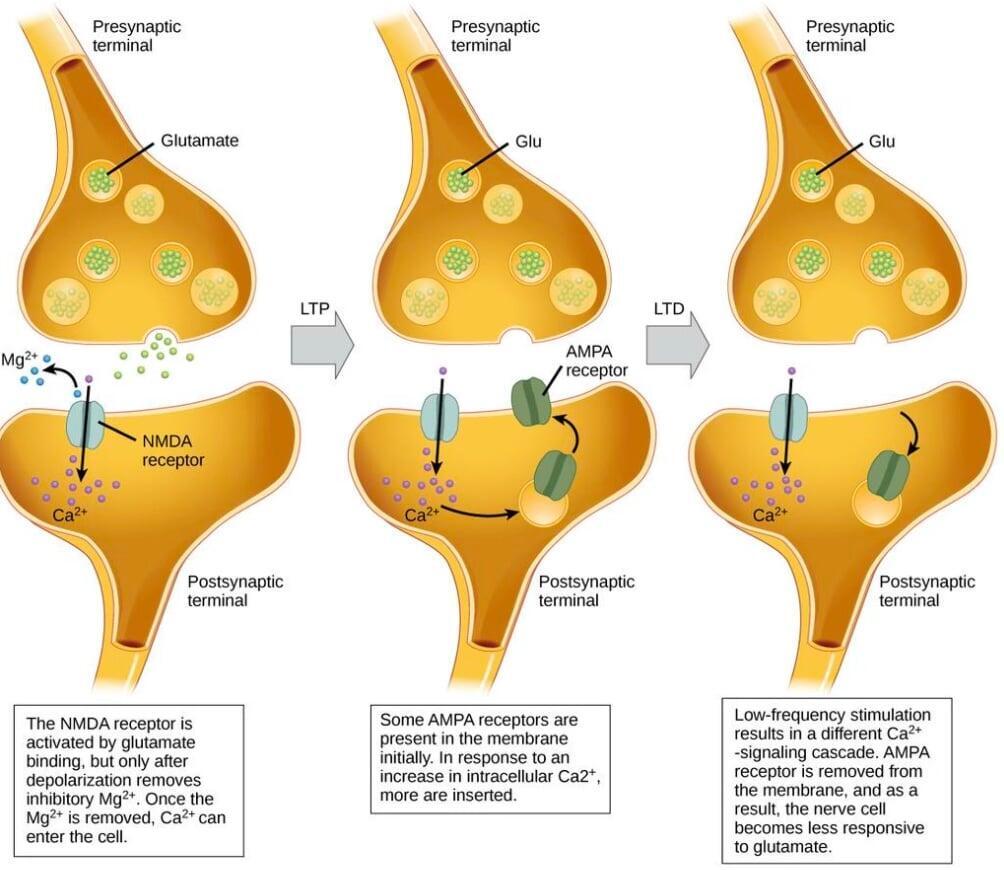
More recently, Carrick demonstrated in a double blind randomised controlled trial that eye movement training produced changes in quantitative electroencephalogram patterns and in the NIH Stroke Scale in patients suffering from acute middle cerebral artery ischemic stroke, compared to a control group treated only with aspirin. The conclusion was that the eye movement training could induce altered brain activation to accompany the functionality of saccades. (14). Examples of plasticity at the synaptic level can be illustrated in Figure 2. (15)
Figure 2: Long-term potentiation and depression. Calcium entry through postsynaptic n-methyl-D-aspartate (NMDA) receptors can initiate two different forms of synaptic plasticity: (i) long-term potentiation (LTP) and (ii) long-term depression (LTD). LTP arises when a single synapse is repeatedly stimulated. The stimulation causes a calcium- and CaMKII-dependent cellular cascade, which results in the insertion of more α-amino-3- hydroxyl-5-methyl-4-isoxazole propionate (AMPA) receptors into the postsynaptic membrane. The next time glutamate is released from the presynaptic cell, it will bind to both NMDA and the newly-inserted AMPA receptors, thus depolarising the membrane more efficiently. LTD occurs when a few glutamate molecules bind to NMDA receptors at a synapse (due to a low firing rate of the presynaptic neuron). The calcium that does flow through NMDA receptors initiates a different calcineurin and protein phosphatase 1-dependent cascade, which results in the endocytosis of AMPA receptors. This makes the postsynaptic neuron less responsive to glutamate released from the presynaptic neuron.
Neuroplasticity was shown to be not limited to neural injury and recovery. It includes dendritic remodelling, synapse turnover, long-term potentiation, and neurogenesis. In terms of human welfare, it encompasses brain development, the learning of skills, the formation and loss of memory, and self-repair from neural injuries. (16)
For example, Carrick reported in a trial involving healthy volunteers that manipulation of the second cervical motion segment produced what was evidently an enlargement in the circumferential measurement of the blind-spot map associated with decreased cortical activity in only one cortical hemisphere. In other words, this particular intervention may have been associated with a change in brain function. (17)
Even more intriguing was the observation that changes in hippocampal structure could be found in London taxi drivers as they became familiar with the city’s layout, shown by a redistribution of grey matter compared to controls. (18, 19)
Because models in structural pathology fail to adequately account for several clinical and experimental findings in individuals with chronic musculoskeletal disorders, and because treatments guided by these models fail to effectively treat many chronic disorders, alternative paradigms are being sought.
The model of neuroplasticity, addressing changes in the central nervous system, has been proposed to be the missing link to our understanding of chronic musculoskeletal disorders. (20)
Neurogenesis
Neurogenesis refers to the birth and proliferation of new neurons in the brain, occurring then stem cells located in the dentate gyrus, the hippocampus, and possibly the prefrontal cortex split into a stem cell and a cell that becomes a neuron with axon and dendrites, the latter capable of migrating into an area of the brain where it is needed. For centuries the belief was maintained that the ability of the brain and spinal cord to regenerate was limited to embryonic development, and that damage to these organs thereafter tended to be permanent. But this changed in 1962 when Joseph Altman found that several areas of the rat brain were capable of incorporating radioactive thymidine into the DNA, (21) including the olfactory bulb and dentate gyrus. (22)
Yet interest in brain regeneration languished until 1993, when rat brain stem cells were found to proliferate in vitro by the addition of growth factors, growing into cell aggregates called ‘neurospheres’ which differentiated into neurons and glia. (23) Neuroblasts generated in the subventricular zone of the dentate gyrus were shown to migrate to the adult olfactory bulb and differentiate into neurons, (24) creating the impression that grafted neurons had the potential to migrate within the brain. Neurons have also been suggested under certain conditions to migrate to regions other than the olfactory bulb and dentate gyrus. (25)
It does appear that adult neurogenesis offers the opportunity to learn how neurons integrate into mature brain circuits, (26) while at the same time it appears that altering the environment in which neuronal stem cells may differentiate will not alter the type of neurons that they produce. (27, 28) The fact remains, however, that the human hippocampus retains its ability to generate neurons throughout life. (29)
Neurotransmitters and receptors
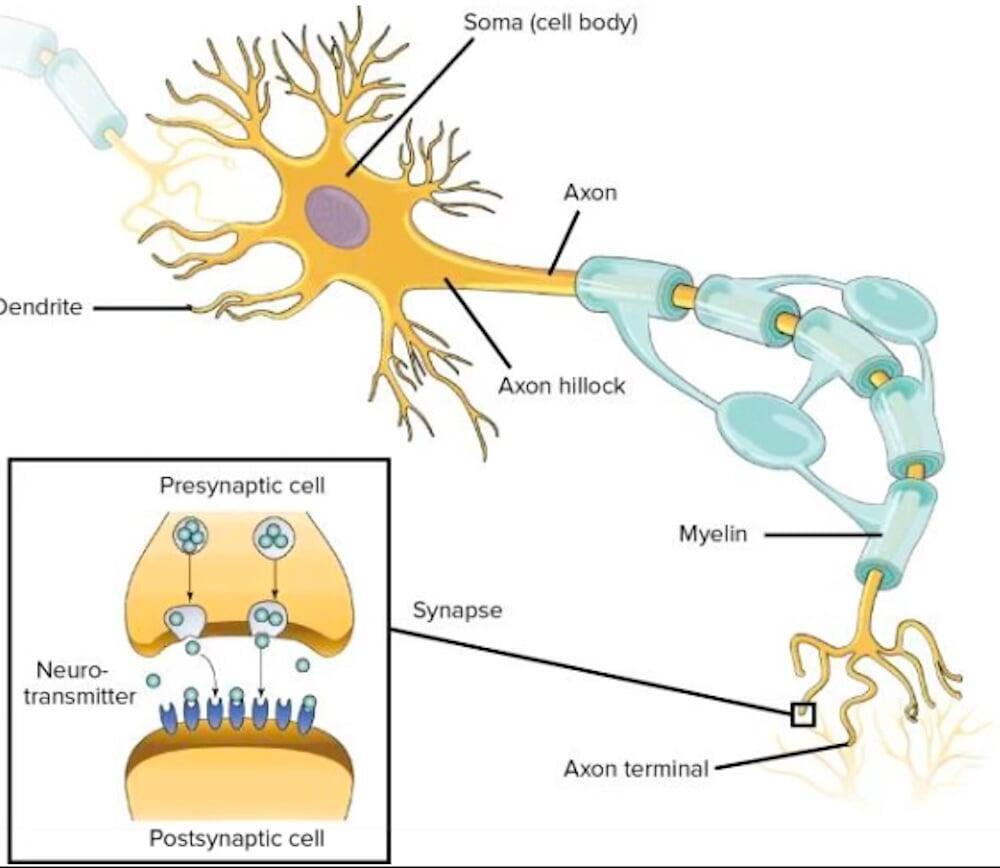
The actual generation of action potentials occurs in a region of the axon known as the hillock area, (30) sending the potential through the length of the axon to its terminal region. Here the potential triggers the release of chemical neurotransmitters into the synapse, a gap which separates the cell from its nearest neighbouring neuron. It is the neurotransmitter which enables the action potential to reach the next neuron in a chain reaction, binding at the neighbouring cell’s surface to specialised receptors which reactivate the action potential through that neuron, as shown in Figure 3. (31)
Figure 3: Structure of neuron and transmission of action potential by neurotransmitters.
The most prominent neurotransmitters involved in neural regulation at the molecular level in functional neurology are, as follows:
Acetylcholine
A closer examination of the role of the neurotransmitters at the synapse provides a biochemical clue as to how the regulation of nerve signalling by molecular intermediates may occur. (32) Using acetylcholine as a typical neurotransmitter, Figure 3 illustrates how:
- The action potential traveling down the length of the axon causes voltage-gated calcium channels to open, leading to the influx of Ca+2 ions from the extracellular space.
- By means of an exocytotic process, Ca+2 releases a neurotransmitter (acetylcholine) from vesicle entrapment, allowing acetylcholine to enter the synaptic (cholinergic) cleft.
- Acetylcholine binds to a specific nicotinic acetylcholine receptor on the neighbouring neuron, raising the resting potential of the postsynaptic nerve or muscle cell, opening a channel for sodium to enter the cell and trigger an action potential as discussed above.
- Numerous poisons may either block acetylcholine from binding to its receptor (curare) or prevent its being recycled into its neuron of origin as acetate and choline (neurotoxins).
This chain of events leads one to suspect that neurotransmitters may be the locus of the regulation of signalling between neurons. To qualify as a neurotransmitter, the chemical must satisfy five criteria: (32)
- It must be produced by neurons
- It must be stored in the synapses
- It must be released into the synaptic cleft upon stimulation
- It must bind specifically to receptors on the postsynaptic membrane of either another neuron or muscle cell, and
- The binding must trigger an ion influx that governs the activity of the target cell.
What we illustrate in Figure 4 represents the basic essentials of but one of the abundant neurotransmitter-initiated pathways of nerve transmission.
Figure 4: Acetylcholine-mediated mechanism of neural transmission. (A) Cholinergic response; (B) Nicotinic acetylcholine receptor; (C) Metabolism of acetylcholine.
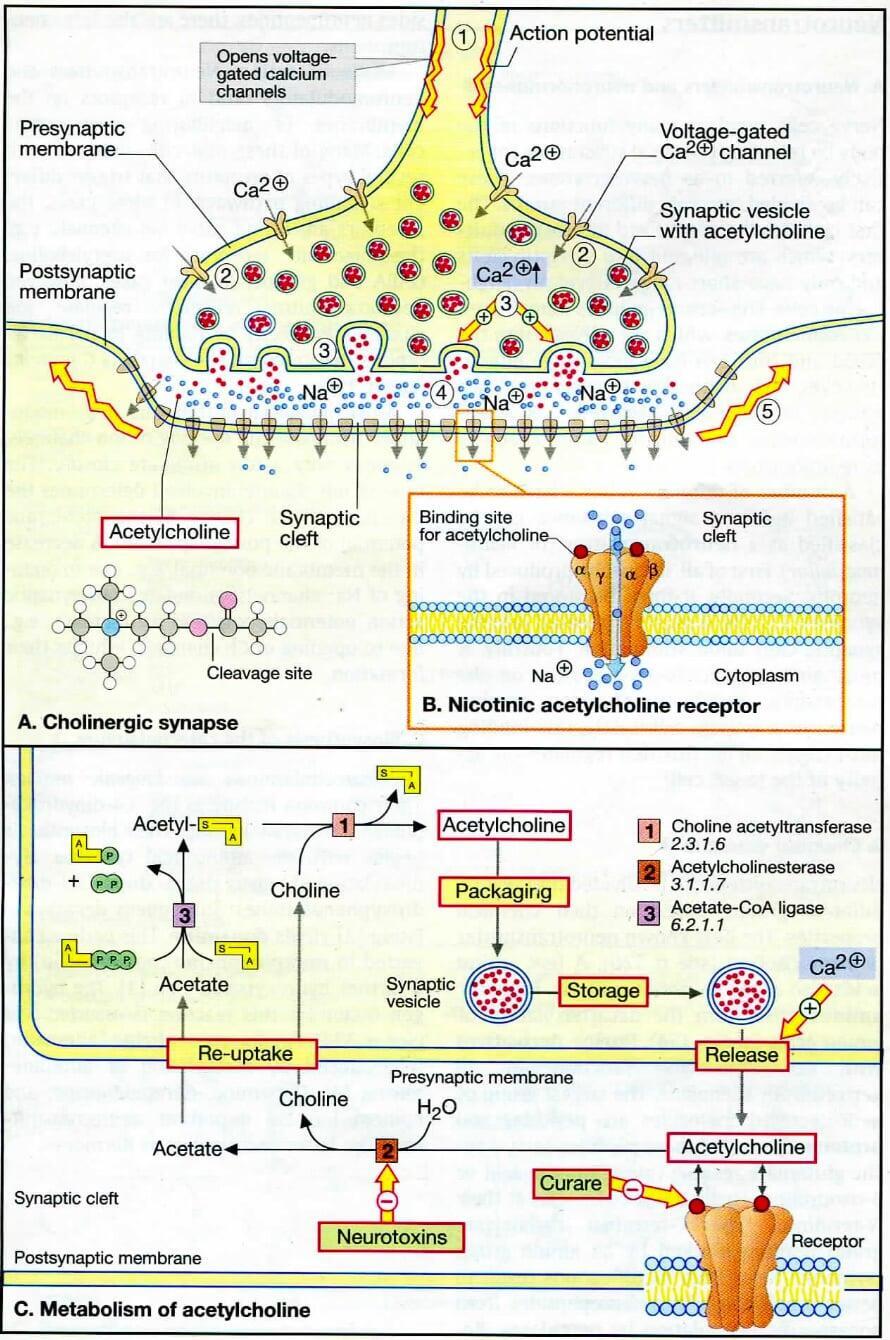
While acetylcholine is the best known neurotransmitter, amino acids, biogenic amines, purine derivatives from adenosine, peptides and proteins are also members of this neuromodulator. Other neurotransmitter-receptor complexes therefore need to be noted as well. The nicotinic receptor as a ligand-gated ion channel functions for gamma-amino butyric acid and glycine as well as for acetylcholine. Most neurotransmitter receptors control ion channels indirectly by binding to 7-helix receptors which transmit the signal via G proteins. The latter, consisting of three dissimilar subunits, allow an exchange of bound GDP for GTP and ultimately generates what is known as a second messenger. Second messengers include cyclic AMP (cAMP), cyclic GMP (cGMP), diacylglycerol, inositol triphosphate, calcium, and arachidonate. Among their other functions is the ability of second messengers to allow signal amplification within the cell.
The end result of receptor stimulation at the synapse is to provoke DNA transcription of appropriate genes to produce proteins and neurotransmitters.
Other products to follow are cytoskeletons, membrane receptors and channels, and enzymes.
Gamma amino butyric acid
A more representative and far more complex neurotransmitter in functional neurology is gamma-amino butyric acid (GABA), which acts as the primary inhibitory neurotransmitter in the mammalian central nervous system, playing a key role in modulating neuronal activity. No less than three classes of GABA receptors exist:
- GABAA: Electrophysiogical studies have indicated that the GABAA-receptor complex rapidly mediates an increase in membrane conductance that is often accompanied by membrane hyperpolarisation. The result of this is an increase of the firing threshold and thus the reduction of spontaneous initiation, leading to overall neuronal inhibition with the membrane potential stabilised to near the resting level. With a damping of postsynaptic depolarisation achieved, there is the reduced likelihood of brain function from overreacting from excessive initiation of action potentials. The GABAergic synapse has been shown to have a far more complex structure than the acetylcholine receptor shown in Figure 4, although the basic mode of action in chemical transmission of signals across the synaptic cleft is essentially the same. (33)
- GABAB: These are guanine nucleotide-binding (G) protein coupled receptors, the function of which is to modulate Ca+2 and K+ channels, capable of eliciting both presynaptic and postsynaptic inhibition. They have a broad range of expression in the nervous system:
- modulating synaptic excitability and placidity in the cerebral cortex
- generating rhythmic activity in cortical and thalamic circuits
- relaying primary afferent input to the spinal cord and brainstem, and affecting the activity of dopaminergic and other monoaminergic neurons. (34) Unlike the fast synaptic acting GABAA receptors, GABAB receptors exert a slow inhibitory potential. (35)
- GABAC: Like their GABAA counterparts, GABAC receptors are linked to chloride channels but are slow rather than fast-acting and also are insensitive to the benzodiazepines and anaesthetics that affect GABAA receptors. (36, 37) Dopamine has been reported to modulate this receptor activity in both catfish cone-driven horizontal cells (38) and tiger salamander bipolar cell terminals. (39)
N methyl D-aspartate
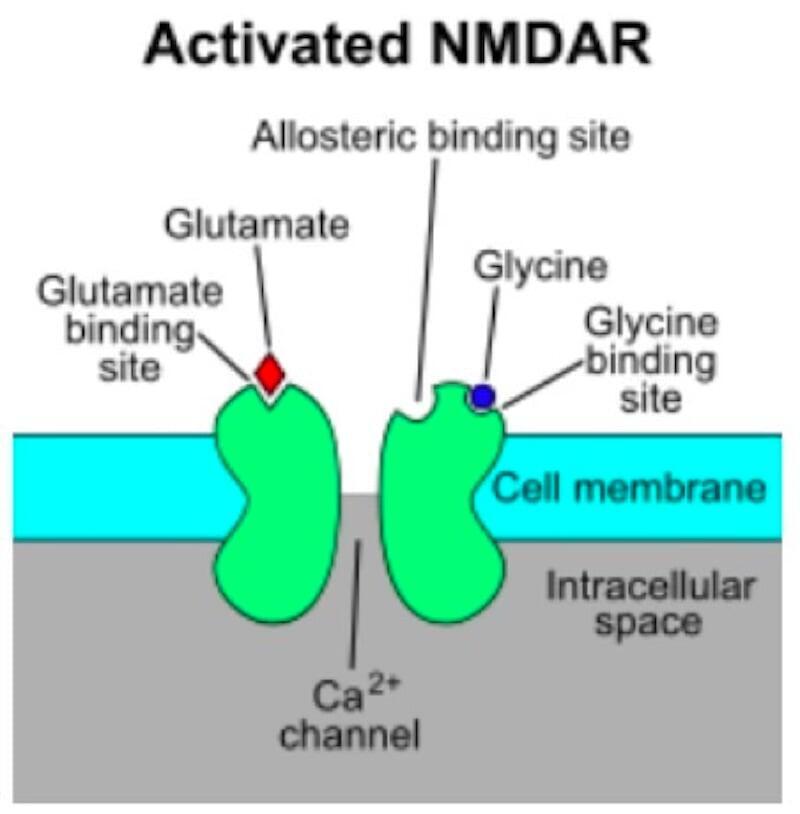
The leading molecular species for controlling synaptic plasticity and memory function has been identified as the N-methyl-D-aspartate (NMDA) receptor. (40) It is so named due to the selective binding of the agonist molecule NMDA to it and not to other glutamate receptors. It is an ion channel protein located in neurons, activated when both glutamate and glycine (or D-serine) bind to it. This allows positively charged ions, such as calcium (Ca+2), to flow through the cell membrane. (41, 42) (Figure 5) The increase of Ca+2 within the cell allows it to function as a second messenger in a variety of signalling pathways. However, extracellular magnesium (Mg+2) (43) or zinc (Zn+2) can bind to specific sites and prevent Ca+2 binding and activation. It is only with depolarisation of the cell that Mg+2 or Zn+2 can be dislodged from the pore, permitting a voltage-dependent flow of Ca+2 or sodium (Na+) ions into the cell and potassium (K+) ions out of the cell. (44, 45)
Figure 5: Activation of the NMDA receptor (NMDAR) by glutamate and glycine, opening channel for Ca+2
NMDA receptors are associated with synaptic plasticity, shown perhaps most directly by the demonstration that extra-synaptic NMDA receptors inhibit long term potentiation while producing long term depression, (46) while the inhibition is prevented by introducing an NMDA antagonist. (47) One of six subunits of the protein identified as NR2B has been pinpointed as a locus of plasticity since the ratio of NR2B to NR2A decreases with age in diverse animal species (including humans) starting on or before sexual maturity. In other words, the relative abundance of NR2B in the juvenile brain appears to confer upon it a greater plasticity than the adult brain.
Interestingly, NMDARs have been identified outside as well as within the synapse. In research conducted over the past decade, the NMDARs outside of the synapse have been found to play a major role in excitotoxicity and cell death, while physiological activation of the NMDARs inside of the synapse can contribute to cell survival. This has led the authors of a review to suggest that preventing excessive activation of the extrasynaptic NMDARs could provide therapeutic benefit in such cases as Alzheimer disease or Huntington disease. (47)
Dopamine
Dopamine belongs in both the catecholamine and phenethylamine families and plays a dual role, serving as
- the primary neurotransmitter in the brain, and
- a local chemical messenger outside of the nervous system. Able to cross the blood-brain barrier, dopamine is confined primarily to: (48)
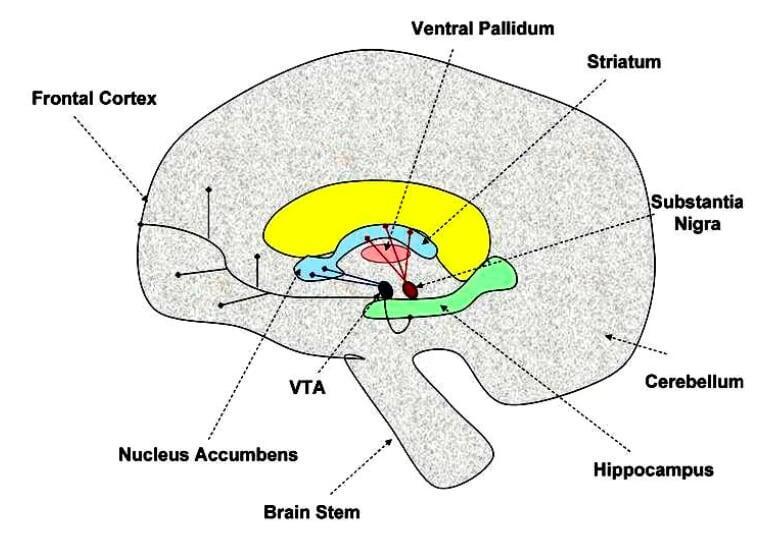
- The nigro-striatal tract, consisting of dopaminergic neurons originating in the substantia nigra projecting into the striatum. This tract is believed to be involved in the control of motor movement,
- The mesolimbic tract, consisting of dopaminergic neurons projecting from the ventral segmental area into the nucleus accumbens, frontal cortex, and hippocampus. This particular region is believed to be involved in motivation, reward, and learning.
These regions are outlined in Figure 6. (49)
Figure 6: Dopaminergic tracts in the brain. RED = nigro-striatal tract; PURPLE = mesolimbic tract; VTA =ventral tegmental area; DASHED ARROWS = specific brain regions; SOLID ARROWS IN CENTER =dopaminergic neuronal tracts
As with most biologically active substances, dopamine exerts its effects by means of specific binding to and activating receptors. Two evolutionary and genetically different subtypes of receptors exist within the dopaminergic system (D1-like and D2-like) with a total of five distinct receptor classes in all. (50) The two receptor classes, when stimulated by a common agonist, produced an increase of intracellular calcium via a signalling pathway that was not activated by either receptor alone or when only one of the co-expressed receptors was activated by a selective agonist. (51) The consequences of the calcium stimulation produce changes in gene expression, protein production, enzyme levels, the cells’ firing rate, and the neuron’s sensitivity to dopamine itself. It begins as the cell uses calcium to build and strengthen synaptic connections to other neurons, releasing the calcium from vesicles stored within the neuron as shown in Figure 4.
The physiological effects of dopamine expressed downstream include the following:
- Gene expression: Immediate early genes that are activated in dopaminergic neurons following stimulation include those of the fos family, (52, 53, 54) fos being a transcription factor that is upregulated in the brain following stimulation from drugs or other rewarding stimuli such as sexual behaviour or exercise. (54)
- Expression of numerous neuropeptides: Dopamine signalling has been shown to have direct effects upon the expressions of:
Substance P (55) Dynorphin (56) Enkephalin (57) Orexin (58)
- Regulation of motor movement control: Purposeful exercise and/or movement that expends a significant amount of energy is regulated by the dopamine system. (59, 60) Derangements of the dopamine system play a central role in the development of Parkinson’s disease (61) and Attention Deficit Hyperactivity Disorder. (62)
- Mediation of behavioural responses to rewarding stimuli: It is generally accepted that the dopamine system is involved in reward and reinforcing mechanisms, as shown by the results of psychostimulant administration. (59, 63) It functions both as the centre of motivation or wanting as well as being directly affected by the physical activity involved in the pursuit of those entities desired. (64, 65, 66)
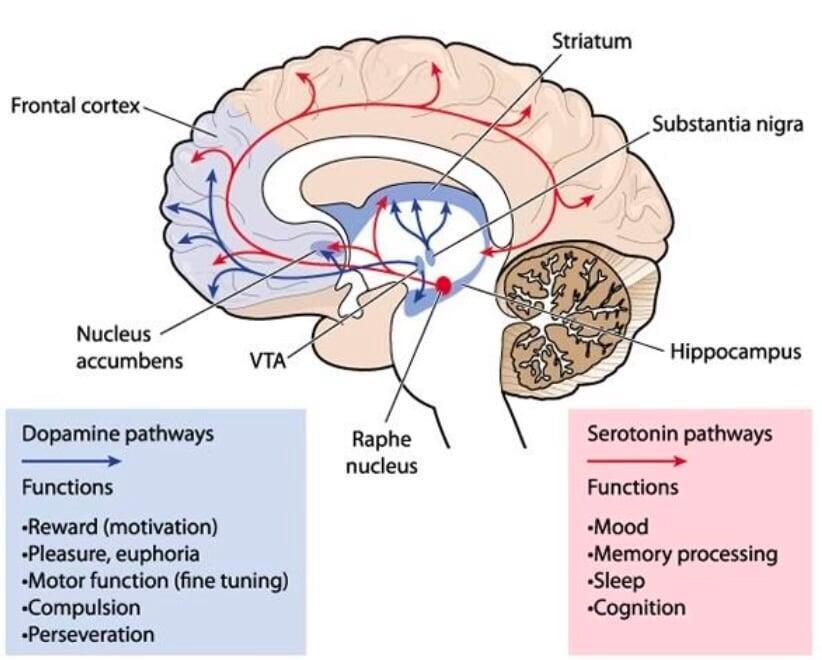
Figure 7 presents an overview of the dopamine pathways in the brain and their downstream effects. (67)
Figure 7: Dopamine and serotonin pathways in the brain and behavioural functions
Serotonin
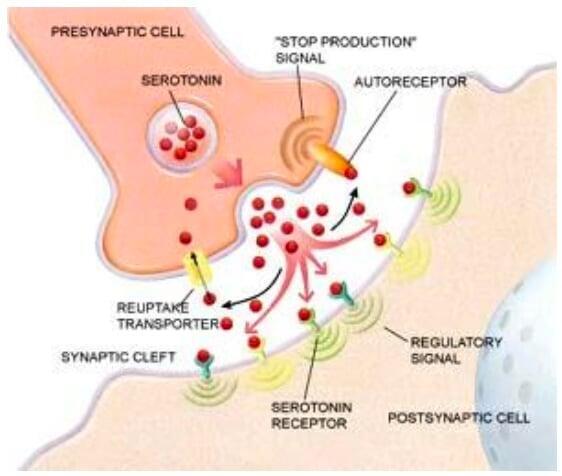
Serotonin (5-hydroxytryptamine, or 5-HT) is a monoamine neurotransmitter with multiple biological effects, synthesised from tryptophan. It is bound to a transporter protein known as 5-HTT located in the presynaptic cell membrane and responsible for the re-uptake of serotonin into its cell of origin after it has been released into the synaptic cleft to signal the adjacent neuron. The length of time that the chemical signal remains in the synapse is determined by the number and activity of the 5-HTT proteins. (68) Figure 8 illustrates these steps. (69)
Figure 8: Function of serotonin and serotonin transporter. Serotonin is released from the presynaptic cell and bound to receptors on the postsynaptic cell. Transporter protein returns serotonin to the presynaptic cell, terminating serotonin action but allowing serotonin to be recycled if it is not metabolised.
Many of serotonin’s function can be described at the molecular level as follows:
- Regulator of mood: The popular conception of serotonin is that it enhances feelings of content and happiness. (70) Indeed, serotonin has a pervasive influence upon brain activity, being released from axons originating largely in the raphe nucleus of the brainstem but spreading into almost all brain areas. This diffuse mode of action differs from the rapid activity at the synapses, as shown in Figure 7, in which extracellular levels of serotonin will be highly sensitive to the rate at which it is removed.
- Modulation of nitric oxide synthase: Numerous lines of evidence suggest that the production of nitric oxide is regulated by the 5-HTT transporter. (71)
- Activation of hypothalamic-pituitary axis: Stimulation of the HPA axis in response to serotonin has been suggested in a mouse model, seen with the abundant expression of serotonin 2C receptors I the paraventricular nucleus of the hypothalamus linked to the activity of corticotropin-releasing hormone. (72)
- Regulation of glucose balance: Serotonin 2C receptors have been shown to improve glucose tolerance and reduce plasma insulin in mouse models of obesity and type 2 diabetes. Downstream activation of melanocortin-4 receptors was identified as the mechanism involved, a matter of possible clinical significance since pro-opionmelanocortin neurons, found in the hypothalamus, are known to play a key role in suppressing appetite and inducing weight loss. (73)
- Regulation of bone metabolism: Gut-derived serotonin regulates osteoblast proliferation and bone formation, while brain-derived serotonin regulates bone mass through the sympathetic nervous system. (74)
In addition to those factors regulating neurotransmitter activity are those pertaining to the neuron itself. These would include an adequate supply of nutrients, cofactors, and essential compounds as well as assuring the sufficient exchange of oxygen and carbon dioxide. Lack of these compromises the production of protein as the result of what is known as transneural degeneration. Resulting from this is the neuron’s initial increase irritability, the elevation of its sensitivity to stimulation. But this hyperactivity can last for only a relatively short period of time in the face of deficient nutrients, so that the loss and degradation of microfilaments and microtubules as well as of membrane integrity allows calcium ions to enter unimpeded, resulting in cell death.
These detrimental effects may then be transmitted downstream in a process known as diaschisis. (6)
It is important to recognise that, while such receptors as those that respond to gravity or which maintain pacemaker depolarisation are constant in nature, most receptor systems are not and are thus periodically activated with surges of activity. The latter would include the cortical cells of vision or of memory which experience interruptions with disuse, such as in sleep or neglect. Yet these neurons are sustained to subthreshold activation by complex multineuron systems. (5)
Neural networks: Excitation and inhibition
Neurons are able to receive signals from up to 10,000 presynaptic neurons and likewise can deliver contacts to a like number of postsynaptic neurons. Understandably, this capability gives rise to enormously complex neuronal circuits. Some of the more basic circuit configurations are shown in Figure 9. (75)
Hyperexcited states of neurons, known as ‘wind-up’, suggests an inappropriate degree of output per unit input. Neuronal damage can result from: (30)
- Overactivation of the NMDA receptors, resulting in cytotoxicity due to increased intracellular Ca+2 concentrations.
- Formation of free radicals from anaerobic energy production pathways, leading to damage to membranes and membrane receptor structures, or to mutations in DNA.
- Transneural degeneration, occurring when intracellular protein and energy stores fall below the level needed to support the increased demands of hyperactivity.
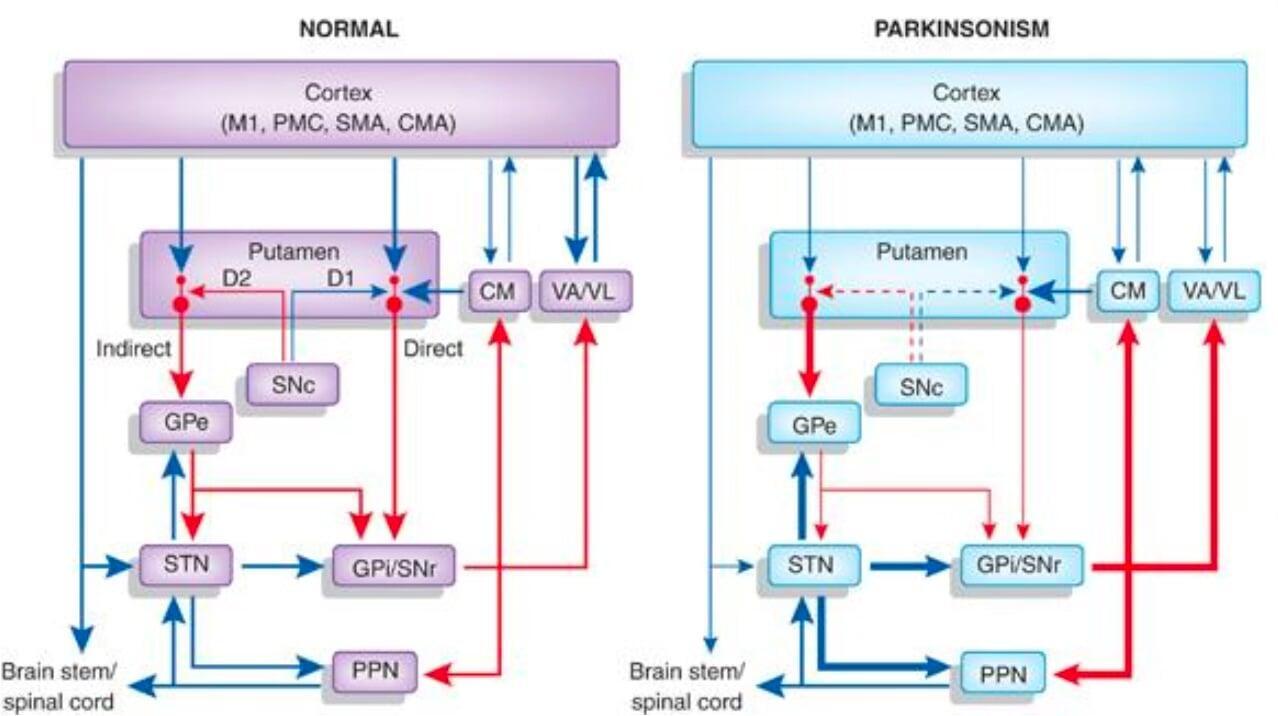
A translation of these networks onto a clinical platform is exemplified by the schematic in Figure 10, in which both the direct and indirect pathways of motor circuits of the basal ganglia are shown in both the normal and Parkinsonian states. (76, 77)
Figure 9: Basic neuronal networks involved in inhibition and excitation of signalling.
A) Feedforward excitation: One neuron relays information to its neighbour, moving the membrane potential closer to the threshold of firing and generating an action potential.
(B) Feedforward inhibition: A presynaptic cell excites an inhibitory interneuron, which then inhibits it next succeeding cell. Its role is to limit or shut down excitation in a downstream neuron by moving its membrane potential away from the threshold of firing.
(C) Convergence/divergence: A postsynaptic cell receives convergent input from multiple presynaptic cells, while any individual neuron can make divergent connections to multiple postsynaptic cells.
(D) Lateral inhibition: A presynaptic cell excites inhibitory neurons, which in turn inhibit neighbouring cells in the network.
(E) Feedback/recurrent inhibition:
(E1): A presynaptic cell connects to a postsynaptic cell, the latter connected to an interneuron which in turn inhibits the presynaptic cell.
(E2): Each neuron in the closed chain inhibits the neuron to which it is connected. This apparently quiescent pattern can lead to complex spike activity.
(F) Feedback/recurrent excitation:
(F1): A presynaptic neuron excites a postsynaptic neuron, which in turn excites the presynaptic neuron, the activation thus being perpetuated.
(F2): A presynaptic neuron excites a postsynaptic neuron, which in turn excites itself either directly or indirectly via other postsynaptic neurons.
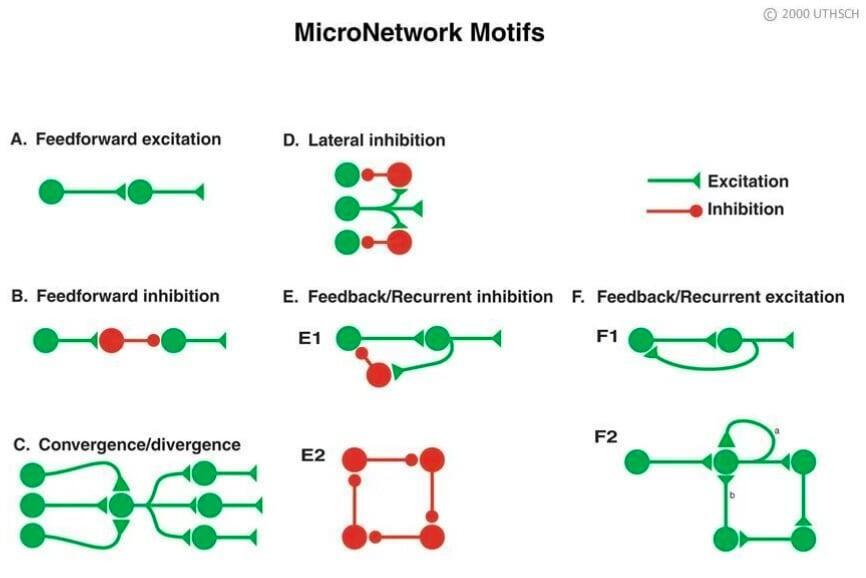
Figure 10: Direct and indirect pathways of the basal ganglia motor circuits in normal and Parkinsonian states.
Red arrows: Inhibitory projections; Blue arrows: Excitatory projections; Changes in arrow thickness represent proposed increases (thicker) or decreases (thinner) in the firing rate activity of specific connections.
Dashed arrows labelling dopaminergic projections D1 and D2 from the SNc to the putamen in Parkinsonism indicate the partial lesion of that system.
Many connections have been omitted from this diagram.
Key:
CM: centromedian nucleus
CMA: cingulate motor area
GPe: globus pallidus, external segment
GPi: globus pallidus, internal segment
M1: primary motor cortex; PMC: pre-motor cortex
PPN: pedunculopontine nucleus
SMA: supplementary motor area
SNc: substantia nigra pars compacta
SNr: substantia nigra pars reticulata
STN: subthalamic nucleus
VA/VL: ventral anterior/ventral lateral nucleus.
Brain hemisphericity
Brain hemisphericity is based upon the finding that the human brain has been described as an asymmetric entity. (78, 79) However, the precise relationship between the brain’s asymmetric design and the functional control managed by each hemisphere remains a controversial subject. As to how much each hemisphere may function is deemed to relay upon its afferent stimulation from the periphery in addition to nutrient and oxygen supply. Current theory holds that hemisphericity is expressed in cortical modulations of the autonomic nervous system, sensory perceptions, cognitive, attentional, learning, and emotional processes. (80) Suggestive evidence was provided in a study of male adolescents of North American native ancestry subjected to a regimen of processing consonant-vowel combinations (CVs) and musical melodies. A laterality index suggested left hemisphere involvement for melodies and more for CV processing. (81) A further hint was provided in a study of normal young women compared to normal young men within a setting that emphasised hypnosis and partial sensory deprivation.
In these surroundings, the women’s reporting of a significantly stronger experience of a ‘presence’ correlated with their higher score on Vingiano’s right hemisphericity questionnaire. (82) Corroboration was offered by Lazure’s finding in a questionnaire administered to 50 boys and girls in grades 9 and 12 that a lower self-esteem score obtained on the Rosenberg questionnaire was associated with greater right hemisphericity, as measured by the Vingiano scale (r=0.52). (83)
It has been suggested that an abundance of right- and left-sided structures in the brain besides the cortical hemispheres may be subject to asymmetric function. These would include the thalamus, amygdala, hippocampus, caudate, basal ganglia, substantia nigra, red nucleus, cerebellum, brainstem, and nuclei. To this assortment of structures might be added the peripheral nervous system.
It has been further proposed that hemisphericity could lead to the dysfunction of major systems of the body, including the spine. Hemisphericity of the latter would include subluxation, spinal stiffness (increased extensor tone), spondylosis, intrinsic spinal weakness (decreased postural tone), decreased A-P curves in the cervical and lumbar spine, increased A-P curves in the thoracic spine, increased postural sway in sagittal or coronal planes, and pelvic floor weakness. (6)
Effects of modalities upon neuroplasticity and neurogenesis
These interventions are built on the premise that functional synaptic connections are built involving cortical and subcortical (striatal and cerebellar) structures, following exposure to a variety of motor experiences. The connections are proposed to be highly dependent upon sensory information. (84)
Rehabilitation
This approach addresses specific areas that are affected by a neurological deficit leading to over- or under-activation. The focus is upon the root cause rather than symptoms and includes the following forms suggested by one clinic specialising in functional neurology: (85)
Optokinetic (eye movement) exercises:
A trial involving patients with left-sided chronic neglect (impaired or lost ability to react to or process visual, auditory, tactile, or olfactory sensory stimuli) subjected to repetitive optokinetic stimulation with active pursuit eye movements (R- OKS) compared to a cohort undergoing conventional visual scanning (VST) revealed superior effects experienced by those in the former group in all tasks (digit cancellation, visuoperceptual and visuomotor line bisection and visual size distortion). (86) A larger randomised trial of healthy subjects found that those subjected to OKS exposure for five consecutive days displayed significant reductions of visual dependency, both at a perceptual and postural level, compared to a nonintervention control group. (87) A more elaborate follow-up clinical trial conducted by the same lead author found that patients with a clinical diagnosis of a peripheral vestibular disorder or chronic dizziness and/or unsteadiness responded positively to a more economical unsupervised DVD that provided an optokinetic rotating disc or drum, but only for vestibular-visual vertigo, and autonomic symptoms. Posturography and functional gait assessments were superior for groups trained with a full-field visual environmental rotator or supervised cohorts. In any case, optokinetic training provided improvements to individuals experiencing peripheral vestibular disorders. (88)
Balance and coordination therapy:
The goal of this intervention is to provide a balance board or platform in order to increase the activation of the cerebellar structures controlling posture, head and eye yoked movements, and core stability. Support for this approach was offered by Rhyu, who analysed brain MRI scans of 16 male professional speed skaters, comparing those to scans of 18 non-skaters who did not engage in regular exercise. Skaters were shown to possess larger right hemispheres of the cerebellum and vermian lobules VI-VII (the lobes connecting the left and right parts of the cerebellum) than non-skaters, suggesting that the specialised abilities of balance and coordination in the skaters were associated with flexibility in the cerebellar structures.
Specifically, the balance on the right foot required of speed skaters activated the right lobes of the cerebellum, in addition to the effects of learning a visually guided task believed to occur in the right side of the brain. (89) A second investigation involving traumatic brain injury patients found that balance training using PC-based portable balancers with real-time visual feedback induced plastic improvements in balance control which were associated with alterations in the cerebellar white matter microstructure. (90)
Elsewhere, patients with cerebellar ataxia who participated in a home-based balance exercise program displayed significant rehabilitative improvements that were retained in most outcome measures one month later. (91)
Complex movement exercises:
Because specific movements are targeted to specific areas of the brain, exercises which activate areas of the brain that are deficient or over-activated are indicated as a component of functional neurology rehabilitation. Intensive training, for example, is known to produce functional and structural neuro-adaptations. Professional handball players, for instance, displayed an increase in grey matter volume in hand areas, while ballet dancers revealed increases of the grey matter area in foot areas. Fractional anisotropy of the corticospinal tract (FA), on the other hand, showed lower FA in fibres connecting the foot compared to the hand areas of ballet dancers, while handball players revealed lower FA in fibres connecting the hand compared to their foot areas. (92)
A separate investigation involving young adults aged 21-26 revealed modulations of the average activity in the alpha and beta frequencies in EEG patterns of the frontal and central brain regions when subjected to walking conditions combined with a cognitive or motor interference task, indicating an increased cognitive load during the walking In other words, impaired motor performance during dual-task walking was reflected by neural activation patterns of the brain. (93)
After the acquisition of visual motor skills in yet another trial, participants experiencing exercise regimens displayed improvements in procedural memory, but those increases diminished with increasing time lapses between the exercise and acquisition. (94)
A fourth investigation found that moderate dancing activity compared to a non-sedentary control cohort without any dancing experience failed to display significant differences in four cognitive domains or brain volume, suggesting that a critical level of physical activity and fitness may have been attained in the control group. (95)
Vestibular rehabilitation:
The vestibular system (inner ear and cerebellum) are the target areas of this aspect of functional neurological rehabilitation. Included in this type of therapy are a variety of forms of stability exercises, patterned movements of the extremities, rotational forms of movement, and eye exercises. (85)
A systematic review of 9 randomised controlled trials of varying quality revealed positive results in favour of vestibular rehabilitation regarding postural control, functional capacity, and quality of life in an elderly and middle-aged population with complaints of vestibular syndrome, lightheadedness or dizziness. Despite the fact that four studies were rated to be of adequate quality according to the PEDRO scale, they were subject to bias since they did not present allocation concealment or blinding of participants, therapists, or assessors. (96)
In a nonrandomised controlled trial with 20 patients diagnosed with vestibular diseases, cervical manual therapy and shoulder girdle exercises together with head movements, eye coordination tasks, and overall body movements and balance tasks produced improvements in quality of life, postural balance, and intensity of dizziness.These improvements were not associated with pharmacologic treatment. (97)
A novel approach was offered by a team of investigators from Laval University, who determined that the presentation of virtual reality treatments of at least 150 minutes of cumulated exposure ensured symptom improvements in patients with vestibular disorders. The effect was dose-dependent and was based upon the Dizziness Handicap Index and perception of handicap symptoms. (98) A review of the literature led Lacour and Bernard-Demanze to propose a series of general recommendations regarding the timing, type, intensity, and duration of vestibular rehabilitation therapy. They proposed that: (99)
- Therapeutic progression must proceed from the head to locomotion in a top-down sequence of exercises.
- The therapy must address all facets of the vestibular syndrome; i.e., the postural, oculomotor, and perceptive symptoms following vestibular injury.
- Prior to the therapy, nausea, vomiting, and vertigo need to be stopped or reduced.
- Antiemetics and anti-vertigo drugs might be useful in the early (2-3 day) stage after vestibular injury but must be stopped thereafter.
- Regaining eye motion control and eye-head coordination are the primary goals of the therapy.
- Sensory substitution and sensory addition are tools for compensating vestibular loss.
- Recovery of balance control and gaze stabilisation is attained differently among patients; therefore, a stereotyped vestibular rehabilitation protocol is to be avoided.
Developmental disorder rehabilitation:
Areas of the brainstem which are origins of such developmental disorders as Autism Spectrum Disorders, ADHD, learning disabilities, and dyslexia may be targeted for rehabilitation approaches based on the principle of neuroplasticity. Treatments could include eye movement exercises, tracing therapy, complex movement exercises, hand-eye coordination exercises, music therapy, light stimulation, or balance or coordination work. In animal models, a large body of research has demonstrated the effects of environmental enrichment on both brain and behavioural development. Specific indicators have included the weight and thickness of the cortex, the density or affinity of neurotransmitter receptors, and increased numbers of synapses as well as the density of dendritic branching.
The literature has extended to aberrant genes coding for defective neurotransmitters and receptors in the brain leading to disorders of the synapse in autism, raising the possibility that interactions with environmental factors may influence these components and susceptibility to autism. (100)
A closer inquiry into brain anatomy and the ability to learn nonnative speech sounds found that faster phonetic learners appeared to have more white matter in parietal regions of the brain, particularly in the left hemisphere. The authors concluded that morphological correlates of phonetic learning were related to the ability to process rapid temporal variation. (101) Further support of the neuroplastic responsiveness of the brain to interventions addressing developmental disorders was provided in a study of children with dyslexia. After training, performance on both oral language and reading tests significantly improved, bringing the dyslexic readers’ scores into the normal range. At the same time, increased metabolic activity was found in fMRI scans in the left hemisphere language regions, bringing brain activation in these regions closer to that seen in normal children with normal reading skills. (102)
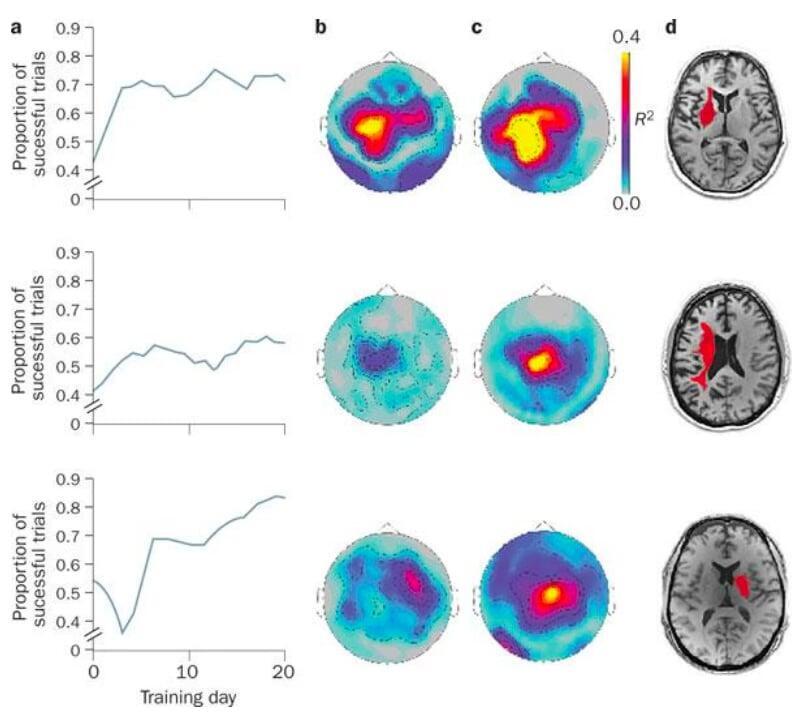
Virtually the same results were obtained in a second study involving dyslexic adults, likewise demonstrating how an external intervention (phonological training) produced increased fMRI signalling in the left hemisphere regions which are engaged by normal readers. (103) Results such as these have led researchers to introduce a cognitive training regimen as a treatment option for ADHD, called Online Neuroplasticity-based Training for the Remediation of ADHD in Children (ONTRRAC), currently under evaluation in a randomised controlled feasibility-efficacy trial. (104) Indeed, a similar brain-computer interface training program for adults with chronic hand hemiplegia after stroke has been shown in 3 patients to increase performance (moving a cursor on a screen) while enhancing MRI images reflecting the modulation of cortical activity, as demonstrated in Figure 11: (105)
Manual medicine (spinal manipulation and cranial therapy)
Nearly 40 years ago, Korr proposed that biomechanically induced deformations of spinal nerves in spinal manipulation could alter axonal transport and with it, trophic influences upon target and effector cells. (106) Analgesia produced by stimulation of neurons outside the customary dermatomal and myotomal distributions used in musculoskeletal diagnosis has been labeled noxious inhibitory control. (107)
The experiments of Sato and Swenson in rats showed that manual therapy could trigger changes in sympathetic function with the potential to alter pain through the sympathetic nervous system’s ability to change afferent input. (108) In healthy humans, diversified cervical adjustments appeared to result in parasympathetic responses seen to dominate the LH/HF ratio in heart rate variability measurements, whereas thoracic adjustments led to a reduction of pulse pressure suggesting a sympathetic response. (109) Depending upon which whether the ipsilateral or contralateral side is treated by manipulation and the cortical hemisphericity of the patient, an increase or decrease in brain function has been reported. (17) From these findings, it could be established that manual therapy activates endogenous analgesia systems.
Figure 11: Modulation of cortical activity in stroke patients by brain-computer interface training. Patients with chronic hand hemiplegia after stroke were trained to move a cursor on a screen via modulation of ipsilesional sensorimotor µ rhythm, which was recorded by magnetencephalography.
Successful trials lead to the brain-computer interact opening or closing the patient’s paralysed hand via a mechanised orthosis.
(a) The performance of three patients across sessions indicates that the proportion of successful trials increased over time. The statistical maps for the correlations between sensorimotor µ rhythm amplitude, which was recorded from the sensors above the ipsilesional primary motor cortex, and successful performance at (b) early or (c) late training time points demonstrates modulation of sensorimotor rhythm with brain-computer interface training.
Red and yellow colours identify areas where there was a high degree of correlation. d Single axial images from T1-weighted, high-resolution MRI scans obtained from each patient. Each patient’s lesion is highlighted in red.
Cranial sacral therapy, on the other hand, assumes that:
- The human brain pulsates unrelated to heart rate at about 10-14 cycles per minute.
- A person can feel these pulsations with one’s fingertips at given locations on the body.
- The craniosacral system (cranium, joints, sutures, and sine) can move and be moved by touching and massaging.
- Restrictions of the natural movements of the cranial system restrict or prevent the flow of cerebral spinal fluid.
- Persons with increased inflammatory levels and neurological activation, such as with Autism Spectrum Disorder, experience restrictions that create learning disabilities, autistic symptoms (such as behavioural problems, poor social relationships, communication difficulties, and poor abstract thought), and other social and intellectual abnormalities.
- With a pressure of about 5 grams, therapists can remove restrictions and generate movement of the cranial system that results in improved functioning.
A publication from the Cambridge Centre for Behavioural Studies in 2011 concluded that the conceptual foundations upon which craniosacral therapy was based ‘have been shown to be flawed and are not substantiated by medical science. Its effectiveness in improving problems to which it has been applied has not been proven scientifically’. (110) More recent publications, however, beginning with a systematic review of 7 studies to assess the benefits of craniosacral therapy, (111) have arrived at a substantially more sanguine conclusion. A study of heart rate variability, for instance, found that patients with subjective discomforts treated with craniosacral therapy displayed increases of standard deviations of all RR-intervals as well as the total power of RR-interval variability in a given frequency range, indicative of a favourable effect of test subjects’ autonomic nervous system activity compared to untreated controls. (112)
Furthermore, a survey of patients with Autism Spectrum Disorder published in 2017 disclosed positive responses from therapists, parents, and clients, establishing a basis for conducting further research addressing this encouraging result. (113) Within the space of just 6 years, further positive responses to craniosacral therapy were reported for patients with chronic neck pain, (114) chronic low back pain (the latter two investigations being randomised sham-controlled trials), (115) migraine headache, (116) and anxiety and depression in patients with fibromyalgia. (117)
The previous conclusion that craniosacral therapy lacks a foundation or scientific evidence to affect patient responses or influence the nervous system (110) thus appears to be premature.
Acupuncture
Documentation of the relationship of neuroplasticity to acupuncture has reached the point at which an entire issue of the journal Neural Plasticity has been dedicated to that single topic. (16) Pathologies of a variety of disorders, such as stroke, Alzheimer’s disease, and pain are related to neural plasticity. The fact that these conditions have been documented to be relieved by environmental stimulation, as will be illustrated by the following examples, simply underscores the connection between acupuncture and neuroplasticity.
- Stroke: In a comparison of 28 right-hemispheric stroke patients and 20 healthy subjects undergoing functional magnetic resonance imagining, stroke patients revealed a decreased functional connectivity between the bilateral motor cortices compared with healthy subjects. The decreased functional connectivity was significantly enhanced after acupuncture at the GB34 point, the most significant active point during the left passive thumb-to-index task. The result was thought to shed light upon the mechanism of neural plasticity for acupuncture therapy. (118) In a rat model of ischemic stroke produced by occlusion of the middle cerebral artery inducing cognitive deficit, lesions could be found by MRI analysis in the cortex, hippocampus, corpus striatum, and thalamus regions, accompanied by learning deficits in a water maze and reductions of the dendritic density in the spine and of synapses in the hippocampal pyramidal cells.. Electroacupuncture at the DU20 and DU24 acupoints reversed all of these changes, as well as increases in mRNA/LIMK1 signalling. It was apparent from these data that the mRNA/LIMK1 signalling mechanism was involved in the electroacupuncture-induced hippocampal synaptic plasticity, contributing to improving the learning and memory during the recovery stage of ischemic stroke in this animal model. (119)
- Experimental spinal cord injury: After spinal cord injury was induced in experimental rats, the motor function of the hind limb was suppressed together with the level of a protein (neurotrophin 3 [NT-3]) essential to neuron survival and growth. Electroacupuncture at the Dazhu (GV 14) and Mingmen (GV acupoints, judged in Traditional Chinese Medicine to stimulate Yang meridians, restorations of both hind limb function and NT-3 levels were found. The conclusion was that the acupuncture treatment promoted neuronal function recovery which could have resulted from upregulating the expression of NT-3.120
- Renal sympathetic activity: In experimental rats, daily acupuncture at the LR3 acupoint for 2 weeks attenuated increases of mean blood pressure that had previously been caused by enhanced renin release. It also increased the ratio of the low-frequency component compared to the high-frequency component in heart rate variability measures while reducing kidney epinephrine and norepinephrine, indicating the reduction of renal sympathetic activity. (121)
- Pain memory: In yet another rat experimental model, electroacupuncture at the bilateral acupoint ST36 alleviated the retrieval of pain induced by the injection of carrageenan, while the NSAID drug indomethacin did not. Injection of a protein kinase (PKA) inhibitor into the anterior cingulate cortex likewise blocked the retrieval of pain memory. Electroacupuncture reduced the activation of PKA together with cyclic AMP (cAMP) and the signalling protein CREB. It thus appeared that electroacupuncture’s suppression of pain memory could be attributed at least partially to the inhibition of the cAMP/PKA/CREB signalling pathway. (122)
- Downregulation of NMDA receptor: Previous data had shown that the N-methyl-d-aspartate receptors (NMDARs) are responsible for the glutamate-induced excitotoxicity in the postischemic brain. Expression of a subunit (NR1) of the NMDAR has been shown to be suppressed by electroacupuncture in a rat model of ischemic stroke, whereas a component of the cell signalling pathway (TrkA) leading to nerve growth factor, critically involved in cell survival and neuroprotective effects, is upregulated. These two factors may be components of the neuroplastic effects of acupuncture in alleviating stroke symptoms. (123)
- Neuroplasticity changes in the human motor cortex: An acupuncture session involving 10 acupoints produced changes in potential amplitude measured by transcranial magnetic stimulation from both the ipsilateral and contralateral hemispheres compared to baseline. Thus, corticomotoneuronal excitability and interhemispheric competition could be modulated by acupuncture therapy in healthy subjects. (121)
Biofeedback
Biofeedback is another mechanism by which environmental stimulation can be utilised to take advantage of the neuroplasticity that characterises human nervous systems. Whereas training and learning could involve numerous mechanisms and areas of the brain affected, biofeedback targets only a specific region of the brain, and thus permits insight into that specific area and how it contributes to behaviour. Several lines of evidence demonstrated the efficacy of biofeedback and its relationship to neuroplasticity:
- Inductions of activity patterns achieved with a decoded functional magnetic resonance imagining (fMRI) signal as an online feedback method were able to accomplish the induction of activity patterns in the visual cortex of healthy adults. This indicated that the adult early visual cortex was so plastic that mere repetitions of the activity pattern corresponding to a specific feature of the cortex was sufficient to produce visual perceptive learning of a specific orientation, even without
- presentation of the stimulus
- conscious awareness of the meaning of the neural patterns that subjects induced, or
- knowledge of the intention of the equipment utilised. (124)
- A second trial, also using fMRI based neurofeedback using blood oxygenation signals from a circumscribed region of interest in the brain demonstrated that participants showed enhanced perceptual sensitivity only if they had undergone the previously learned regimen, and only for that region of the visual cortex. (125) Both studies thus demonstrated a causal relationship between the altered activity in the early visual cortex and the observed behavioural changes. (126)
- A third investigation employing electroencephalogram (EEG) biofeedback administered to post-cancer patients with cognitive impairments showed reductions of the negative cognitive impairments and emotional sequelae of cancer treatment, in addition to improving fatigue and sleep patterns. (127)
- Elsewhere, a neurofeedback training protocol designed to improve sustained attention induced increases of fractional anisotropy in white matter pathways and of the volume of gray matter in cerebral structures involved in the types of increased auditory and visual attention achieved. The authors reported that, after 50 years of research in the field of neurofeedback, this was the first empirical demonstration that neurofeedback training could lead to microstructural changes in white and gray matter. (128)
- A Cochrane review of 13 trials involving 269 people subjected to electromyographic biofeedback showed a small amount of evidence suggesting that the procedure had a beneficial effect when used with standard physiotherapy techniques. Some studies, however, found no effect. (129)
Aromatherapy
With its use of essential oils from plants, aromatherapy is postulated to work by stimulating olfactory receptors in the nose, communicating with the amygdala and hippocampus in the brain which controls emotions and memories. Aromatherapy also acts through the skin.
- The presentation of three different odorants (spiced apple, eucalyptus, and lavender) to subjects produced widely differing alpha and theta activity of the electroencephalo-graphic (EEG) patterns in the left and right hemispheres. These did not agree with self-reports registered on questionnaires, indicating that the perceptual component of olfaction accounted for a limited part of the central nervous system changes produced by smelling an odor. (130)
- Valeric acid (rated as unpleasant) and phenylethyl alcohol (rated as pleasant) were rated as to their effects upon the EEG frequency bands theta, alpha 1, alpha 2, and beta 1 at eight locations. Within 8 seconds after stimulus release, valeric acid increased alpha 2 power whereas phenylethyl alcohol did not. These data indicated that smelling an unpleasant odor led to a cortical deactivation. (131)
- A 1.5-2.5-fold increase in relative sympathetic activity, representing the low frequency amplitude of systolic blood pressure, was produced in humans by the fragrance inhalation of essential oils, such a pepper oil, estragon oil, fennel oil, or grapefruit oil. On the other hand, the fragrance inhalation of rose oil of patchouli oil produced at 40% decrease in relative sympathetic activity. Inhalation of the odorless solvent triethyl citrate caused no change. Inhalation of pepper oil also caused a 1.7-fold increase in plasma adrenaline concentration, while the fragrance inhalation of rose oil led to a 30% decrease of the adrenaline levels. Thus, it was apparent that fragrance inhalation of essential oils could modulate sympathetic activity in adults. (132)
- An early component (at 400-1000 ms) of the beta wave variation, part of an EEG method of measuring the slow brain waves (>13 Hz) at the front of the scalp, was identified as responsive to odor while nearly independent of the subject’s psychological state, degree of arousal, sex, age, or level of consciousness. (133)
- Elsewhere, inhalations of a variety of fragrances by healthy volunteers showed that prolonged inhalations of fragrances influenced autonomic nervous system parameters (as shown by systolic and diastolic blood pressures) as well as mental and emotional conditions. In addition, the chemical chirality of the odor molecules limonene and carvone produced differing physiological responses. (134)
- In percutaneous artery intervention patients in an intensive care unit, aromatherapy oils effectively reduced their anxiety levels and increased the sleep quality, although blood pressure levels were not significantly affected. (135)
Functional neurology massage
Using learning and feedback principles of neuroplasticity, functional neurology massage seeks to produce an improved congruence of the body, its emotions, and the nervous and endocrine systems. Unlike conventional massage, functional neurology massage may employ eye movements, aromatherapy, standing single leg exercises, massage to one side of the body, or light touch bodywork. (136) The purpose is to engage the nervous system, in which several lines of evidence either directly or indirectly suggest a neuroplastic response to massage:
- A study of healthy adults subjected to pressure massage tracked the high- and low-frequency components (HF and LF) of heart rate variability as well as the LF/HF ratio as noninvasive markers of the autonomic nervous system. An increase of the HF ratio after moderate pressure massage suggested increased vagal efferent activity, while the decrease in the LF/HF ratio implied a shift from sympathetic to parasympathetic activity. Interestingly, light pressure massage produced precisely the opposite results. (137)
- A combined regimen of massage and stretching in fibromyalgia patients after 18 sessions produced an increase of parasympathetic and decrease of sympathetic tone shown by heart rate variability. Joint flexibility also improved significantly. (138)
- Similar results were found in children hospitalised in an intensive care unit. Foot and hand massage of 18 children produced a significant increase of parasympathetic activity as seen with a greater increase of HF compared to LF. Interestingly, the sum of HF + LF was positively correlated with clinical severity. (139)
- The combined application of heat and massage for 40 minutes daily, 5 days a week for 2 weeks in 139 healthy subjects led to a significant increase of latency of a sympathetic skin response test, Plasma cortisol and norepinephrine levels also registered significant decreases, the sum total of indicators suggesting a relaxation of the autonomic nervous system. (140)
- A more direct effect of massage was found with rats following facial nerve transection and immediate microsurgical repair. Those animals receiving 5 minutes of daily massage to the left whisker pad throughout the recovery period showed improved functional recovery in all whisking parameters compared to controls. In other words, massage produced an accelerated recovery. (141)
- A similar investigation of the rat transected facial nerve model should that gentle stroking of the paralysed facial muscles resulted in full recovery of function, whereas electrical stimulation failed to improve vibrissal motor performance. (142)
Yoga
Yoga is linked to neuroplasticity through habituation of the posture, breathing, guided imagery, and meditation that characterise this rapidly growing practice. It is essentially a training of the brain to focus as well as process positive thoughts, leading to activation of the parasympathetic nervous system with deeper breathing. The combination of breath control, posture, and presence practiced in yoga encourage a linkage between neural pathways, creating strong and complex neural networks, giving rise to the popular expression, ‘Neurons that fire together, wire together’.
Deep breathing, music, physical activity, communal experience, and music experienced in yoga stimulate the reward system characterised by dopamine and endorphin release which further amplify states of healing and well-being. Specific examples of the neuroplastic and neuro-protective effects of yoga include:
- A study with non-suicidal outpatients of depression offered yoga showed correlated decreases of the Hamilton Depression Rating Scale and increase in serum brain-derived neurotrophic factor. These effects were not seen in groups receiving antidepressants alone or in combination with yoga. The conclusion was that neuroplastic mechanisms could be related to the therapeutic mechanisms of yoga in cases of depression. (143)
- Yoga mediation practitioners were shown in another study to possess greater grey matter volume in frontal, limbic, temporal, occipital, and cerebellar regions compared to a matched control group. A dose-dependent effect was shown by the correlation of grey matter volume with the duration of yoga practice. Furthermore, the yoga practitioner group showed significantly fewer cognitive failures on the Cognitive Failures Questionnaire. From these results, it appeared that hatha yoga practice could be associated with the promotion of neuroplastic changes in executive brain systems, which could confer therapeutic benefits that accrue with repeated practice. (144)
- Essentially the same result was obtained in a second study, in which subjects lacking yoga experience displayed the well-documented age-related global brain grey matter decline, while individuals taking yoga did not. Again, there was a dose-dependent correlation of years of yoga experience with grey matter volume differences in the left hemisphere (frontal operculum and orbital cortex), suggesting that yoga tuned the brain toward a parasympathetically driven mode and positive states. The combination of postures and meditation contributed mostly to the size of the hippocampus, precuneus/PCC, and S1/SLP, while the combination of mediation and breathing exercises contributed the most to V1 volume. The neuroprotective effects of yoga were suggested to provide a neural basis for its beneficial effects. (145)
- In type 2 diabetic subjects aged 30-60 years, numerous types of yoga exercises conducted for 30-4 minutes every day for 40 days led to an increase of right hand and left hand median nerve conduction velocity, while the same parameters of the control groups deteriorated over the period of study. A neuroprotective role of yoga against the progressive decay of nerves in diabetes 2 was suggested by these data. (146)
- In a randomised controlled trial, individuals engaged in yoga breathing compared to control subjects displayed an induction of salivary nerve growth factor, a trophic factor involved in the development, maintenance, and survival of the peripheral nervous system and cholinergic neurons of the central nervous system. (147)
Cognitive exercises, visualisation therapy, guided imagery
Batteries of appropriately designed exercises encourage the creation of new synapses and neural circuits, a manifestation of the neuroplasticity thought to characterise areas of the brain. These approaches fall under the headings of cognitive exercises, visualisation therapy, or guided imagery.
Among the exercises and actions suggested to increase cognitive ability are 8 proposed by Bergland:
- physical activity
- openness to experience
- curiosity and creativity
- social connections
- mindfulness mediation
- brain-training games
- sufficient sleep, and
- reduction of chronic stress. (148)
In terms of guided imagery, several investigations shed light upon the ability of such measures to promote neurological activity:
- Perceptions of a visual cue stimulus were found to modify oscillations in the sensorimotor areas specific to hand movements as monitored by EEG patterns. (149)
- Cued motor imagery enhanced motor evoked potentials of selected muscles in both healthy and stroke-affected individuals. Visual cueing was most effective in young people (20-35 years), while auditory cueing was most effective in both healthy and stroke-affected older people (over 55 years). (150)
- A study of healthy volunteers revealed that an application of guided imagery and music stimuli produced increased activation seen by fRMI in five neural regions associated with negative emotional and episodic memory processing. Regions of the brain included the left amygdala, left anterior cingulate gurus, left insula, bilateral culmen, and left angular gyrus. (151)
- Based on the hypothesis that neuropathic pain after spinal cord injury was based on a mismatch between motor commands and sensory feedback, investigators recruited five paraplegic patients to see whether a visual illusion aimed to correct this mismatch reduced pain. Guided imagery produced a slight reduction of pain, but not as great as that achieved by exposure to a mirror in which patients were exposed to virtual walking consisting of a mirror and a film of lower body walking. (152)
- A six-week training in mental imagery for upper limb amputees produced significant reductions in the intensity and unpleasantness of constant pain and exacerbations. This was accompanied by reductions of cortical reorganisations of motor and somatosensory cortices expanding from the lip area to the hand area, as seen by fMRI. (153)
- Interestingly, individuals who were hypnotised experienced the loss of autonomic (heart rate, respiratory frequency, tonic skin resistance, EEG patterns) responses expected during guided imagery that was considered to be neutral. However, the emotional valence of imagery that was judged to be unpleasant overrode the apparent hypnotic block, such that subjects exposed to such imagery experienced changes in the gamma, beta2 and beta 3 activities as well as in heart rate and respiratory frequency. (154)
Eye muscle exercises (Vision Therapy)
The purpose of vision therapy is to improve visual abilities by training the eyes and brain to work together more effectively. Chinese eye exercises, in particular, were developed as a form of massage around peri-ocular acupoints and grounded in theories of traditional Chinese medicine.
- Eye acupressure was believed to improve neural nutrition to the eyes, reducing eyestrain and the possibility of myopia as well as preventing migraine, neuralgia of the trigeminal nerve, conjunctivitis and facial paralysis. (155)
- More recently, 190 schoolchildren aged 10-14 years underwent standard Chinese eye exercises and experienced a reduction in accommodative lag (ability to accommodate near and distant targets) in the short term compared to those who performed sham point eye exercises. It was unclear, however, whether such exercises were sufficient to prevent myopia progression in the long term. (156)
- Exercises directed at accommodation, vergence, and convergence produced vergence and accommodation improvements in the vergence exercises only. (157)
- Yogic eye exercises, consisting of palming, blinking sideways viewing, front and sideways viewing, rotational viewing, up and down viewing, preliminary nose tip gazing, and near and distant viewing, significantly reduced eye fatigue on a group of undergraduate nursing students. (158)
- In terms of cognitive abilities applied to attention and memory, healthy volunteers subjected to rapid serial visual presentations showed greater accuracy in responding to target letters separated by one distractor, as well as in letter identification if they performed active eye exercises consisting of following a white square on a black background while making saccadic eye movements for 18.5 minutes. (159)
- Elsewhere, a prospective randomised controlled trial found that patients with idiopathic cranial nerve VII paresis experienced a greater rate of recovery if they underwent eye exercises for a period of four weeks with improvements in oribicularis occuli muscle strengths. (160)
- Evidence supporting the efficacy of eye exercises in managing convergence insufficiency, improving visual field remnants after brain damage, and developing fine stereoscopic skills was supported in a systematic review in 2005. (161)
Meditation
Mindfulness meditation, defined by Jon-Kabat Zinn as ‘the ability to pay total attention to the present moment with a nonjudgmental awareness of the inner and/or outer experiences’, (162) raises an interesting paradox. Despite casual impressions, mediation actually appears to the neuroscientist as a complex task, involving what appear to be the contradictory tasks of intense concentration and openness to sensory experiences, emotions, and thoughts. Accordingly, meditation processes have been divided into those engaging focused attention (FA) and those involved in open monitoring (OM). FA, therefore, devotes full attention on a given object in a sustained fashion, while OM maintains an awareness of the content of experience from moment to moment, recognising emotional and cognitive patterns.
Specific neural networks and instances supporting the occurrence of neuroplasticity are described as follows:
- Activation of the dorsolateral prefrontal cortex, associated with executive decision making and attention, has been reported across a variety of mediation styles. Increased activation in the cingulate cortex, which plays a major role in integration of attention, motivation, and motor control, has also been noted, as has the activation of the anterior insula involved with the perception of visceral feelings (hunger, thirst, balance, detections of heart and breathing rates). (163)
- In FA meditation, expert meditators with an average of 19,000 hours of practice showed more activation in a network of brain regions typically involved in sustained attention. However, expert meditators averaging 44,000 hours had less activation in response to distractor sounds used to probe the meditation. This inverted u-shaped learning curve suggested that, after extensive FA meditation training, minimal effort was needed to sustain attentional focus. Compared to novices, experts had less brain activation in regions related to discursive thoughts and emotion while showing more activation in the regions related to response inhibition and attention. These variations with hours of practice suggested plasticity in these mechanisms. (164)
- Demonstrations of neural changes during OM meditation was provided by long-term Buddhist practitioners, who registered electroencephalograms with high-amplitude gamma-band oscillations and phase-synchrony during meditation, differing from controls. Specifically, the ratio of gamma-band activity (25-42 Hz) to slow oscillatory activity (4-13 Hz) was initially higher in the resting baseline before mediation for the practitioners compared to controls. During mediation, the difference between the two cohorts increased sharply. (165)
- Differences in positive and negative responses to emotional sounds as shown by fMRI brain activation patterns of novices compared to experts in meditation are shown in Figure 12 from data from Lutz: (166)
Figure 12: Directionality of brain activation. Areas showing a negative (dark blue) or positive (orange) impulse response on average across 10 seconds in responses to all emotional sounds for 15 novices compared to 15 experts in meditation. Top row (A-D) represents one cross-section at Talalrach coordinate z="3" (a fMRI slice of the brain) and bottom row (E-H) represents another cross-section at the Talalrach coordinate z="13.
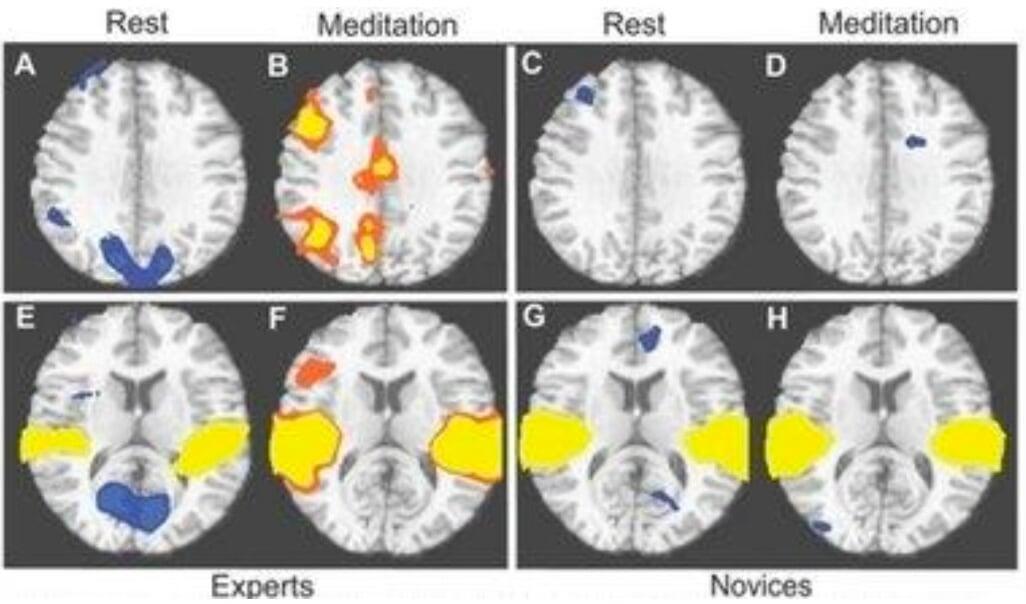
- To assess additional neurological changes during OM mediation an attentional blink test was utilised. It involved presenting two targets T1 and T2 in rapid succession, representing competition between the two targets for limited attentional resources, such that there would be a lack of resources for T2 processing if they were focused upon T1 presented immediately before. After three months of Vipassana OM meditation, the brain-resource allocation to both T1 and T2 was attenuated as shown by diminished P3b amplitudes, suggesting that less elaborate stimulus processing led to the reduced likelihood of ‘getting stuck’ on a target. (167)
- A mindfulness stress reduction program conducted over 8 weeks involving meditation in healthy individuals produced reductions of the density of the right basolateral gray area of the amygdala, a part of the limbic system which performs a primary role in the processing of memory, decision-making, and emotion reactions. (168)
- Increases of gray matter in meditation were apparent from high-resolution MRI patterns of the right orbito-frontal cortex, the right thalamus and left inferior temporal gyrus, and right hippocampus, possibly accounting for the meditators’ singular abilities to cultivate positive emotions, retain emotional stability, and engage in mindful behaviour. (169) A second study showed that brain regions associated with attention, interoception and sensory processing were thicker in meditation participants than in matched controls. (170) Higher gray matter density in the lower brain stem of experienced meditators compared with non-meditators was reported elsewhere. (171)
- Integrative body-mind training, a form of mindfulness meditation, was shown by Tang and coworkers to improve the efficiency of white matter measured by fractional anisotropy in individuals after a 4-week period. It involved increased myelin and other axonal changes, demonstrating white matter neuroplasticity involving the anterior cingulate cortex, a part of the brain network related to self-regulation. (172)
Body movement
The fact that exercise is intimately related with energy metabolism, it is reasonable to suggest that the alterations of energy-related molecular systems should affect neuronal excitability, synaptic plasticity, and cognition. In addition to the hippocampus, which plays a major role in memory processing, the hypothalamus is a brain region influenced by physical activity. The application of exercises to enhance executive function activities, those involved in planning and selecting strategies that organise goal-oriented actions as opposed to basic information processing, has received strong support in the scientific literature as reviewed by Tomporowski and coworkers, who conducted their own review of correlational and cross-section studies as well as randomised experiments to evaluate the impact of chronic exercise or habitual physical activity on measures of children’s mental function. They concluded that gains in children’s mental functioning due to exercise training were found mostly on tasks involving executive functions. (173)
An extensive array of structural and molecular indicators promoting neurogenesis, neuroplasticity, and neural integrity that change with exercise have been identified as follows:
- An increase of gray matter volume and reduced cognitive impairment seen with greater amount of walking. (174) Higher amounts of gray matter tissue density in judo players seen by voxel-based morphometry. (175)
- Increases of hippocampal volume by 2% with aerobic exercise training, effectively reducing age-related loss of volume by 1 to 2 years. (176)
- Elevations of dentate gyrus cerebral blood volume, correlated with measurements of neurogenesis and cardiopulmonary and cognitive function. (177)
- A larger amplitude of ERN, a component of event-related brain potentials (ERPs) which in turn are a class of EEG activity indicative of the synchronous activity of large populations of neurons. This was correlated with greater post-error accuracy of tasks, suggesting increased cognitive flexibility. (178)
- Increased amplitudes of the P3b peak in higher–fit individuals, an ERP component approximately 300-800 ms following stimulus onset. (179)
- Elevations of the neuropeptide brain derived neurotrophic factor (BDNF) in the hippocampus (an area vital for learning and memory), in turn driving several molecular signalling systems involved in the metabolism of energy, thus modulating the capacity of the synapse to process information relevant to cognitive functions. This sequence is illustration in Figure 13: (180)
Figure 13: Proposed mechanism by which exercise may enhance cognitive function by engaging aspects of cellular energy metabolism. Molecular systems, such as µMtCK (myosin-like chain kinase), AMPK (AMP-activated protein kinase), and UCP-2 (uncoupling protein-2) may work at the interface between energy and synaptic plasticity. IGF-1 (insulin-like growth factor), ghrelin and energy-related molecules can interact with BDNF (Brain-Derived Neurotrophic Factor) to modulate synaptic plasticity and cognitive function. (180)
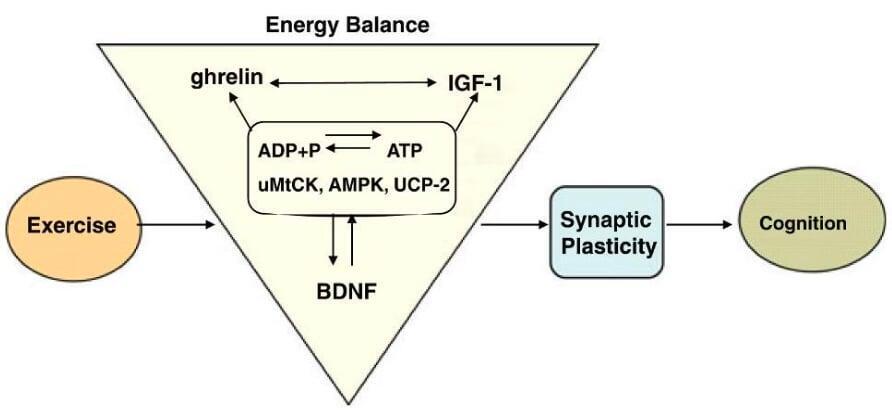
- Promotion of insulin-like growth factor 1 (IGF-1) acting in concert with BNDF, shown by the abolition of the ability of exercise to elevate the levels of BDNF mRNA and protein, as well as exercise’s capacity to augment recall in experimental rats. Investigators suggested that IGF-1 interfaced with BDNF it mediating synaptic and cognitive plasticity,181 lending further support to the schematic shown in Figure 13. (180)
- Identification of vascular endothelial growth factor (VEGF) as a necessary component for the effects of running on adult hippocampal neurogenesis in adult experimental mice. (182)
Together with the aforementioned structural and molecular changes have been an abundance of studies that have documented improvements of cognitive performance with exercise. Cognitive improvements have ranged anywhere from animal performance in a maze to human attention, processing speed, and memory, counteracting the degradations associated with increasing age. (183)
In several instances of diseases or disorders, movement through exercise has been associated with the rebuilding of neural responses, lending further evidence to support the link between movement and neuroplasticity and neurogenesis. The common elements include repetition, intensity, cognitive engagement, challenge, skill training, motivation, goal-based practice, and learning through feedback, all leading to improvements in motor performance as well as cognition. (184)
- In the neurorehabilitation of Parkinson’s disease patients: (184)
- Interventions have included
- treadmill training
- amplitude training
- Tai Chi
- tango dancing
- boxing, and
- forced cycling
- These have all been suggested to restore dopamine with the goal of reconstructing deranged circuitry within the basal ganglia.
- fMRI studies have shown that the learning of dual task training in the rehabilitation of Parkinson’s disease has occurred mainly through compensatory cortical circuits.
- Concerning the restoration of depleted dopamine levels in Parkinson’s disease, studies have demonstrated that exercise can enhance the vesicular release of dopamine, increasing synaptic occupancy and reducing dopamine clearance. Exercise may also enhance the expression of dopamine receptor.
- Additional studies with experimental mice have shown that intensive exercise can restore aspects of glutamate receptor expression. Glutamate and its receptors are known to contribute to neuroplasticity and synaptic strengthening during learning, of possible value in the management of Parkinson’s disease.
- Studies in healthy rodents have shown that exercise increases dendritic spine density in various regions, including the hippocampus and cerebellum. (185, 186) Research to determine whether such findings are applicable to human disorders is clearly indicated.
- An approach to physical rehabilitation called Constraint-induced Movement therapy has been described as having been used ‘effectively’ in managing stroke, spinal cord injury, fractured hip, multiple sclerosis, and cerebral palsy. (187) Brain reorganisation as seen by fMRI has been reported to accompany this therapeutic approach, although it was not clear whether the changes could be detected more in the lesioned compared to the un-lesioned hemisphere in cases of chronic stroke hemiparesis. (188)
- Stimulation timing in stroke rehabilitation appeared to be a critical factor in one investigation, demonstrating that the responsiveness of the motor cortex was affected positively by stimulation during the late motor response period and negatively during the early movement period when the stimulation was combined with a robotic reach practice. This indicated that the sensitivity of the activated motor cortex to additional stimulation was highly dynamic. (189)
- A series of 1 hour Yang style Tai Chi classes with mental imagery conducted twice weekly for 8 weeks with patients with type 2 diabetes led to significant improvements in a variety of functional outcome measures, including Hoffman reflex and sural and perficial peroneal nerve conduction velocity, as well as latency. (190)
Diet
The role of proper diet in maintaining optimal energy metabolism and building materials to the body can be extrapolated without difficulty to the integrity of the neuron, neurotransmitters, and neuroplasticity. Studies of animal and human behaviour and cognition have substantiated the clinical domain of evidence supporting the neuroprotective role of diet, while advances in cell and molecular biology have contributed greatly to conceptualising the constructive roles of diets in promoting neural structure and function.
- Identification of nutrients of interest: An overall list of beneficial nutrients in the human diet has been provided by Gomez-Pinilla, shown below in Table 1: (191)
- n-3 Polyunsaturated fatty acids (3-PUFA, omega-3 fatty acids): 3-PUFAs are distributed to nearly every cell in the body with effects on membrane composition and signalling as well as the regulation of gene expression. Indeed, docosahexaenoic acid (DHA) turns out to be the most abundant omega-3 fatty acid in cell membranes in the brain, while at the same time the human body is not efficient in synthesising DHA and therefore must obtain it from the diet. (191) The role of DHA in neuronal membranes, in particular, has been shown to facilitate membrane translocation activation of the phosphatidylinositol 3-kinase (PI (3)K) Akt signaling, a critical pathway in cell survival. It accomplishes this by increasing phosphatidyl serine (PS), the major phospholipid in cell membranes. This has led Akbar and a team of researchers to propose the mechanism of action of DHA at the membrane level as shown in Figure 14: (192)
- DHA-driven increases in PS with accelerated Akt translocation has been reported elsewhere as well. (193)
Table 1: Nutrients found to affect cognitive function
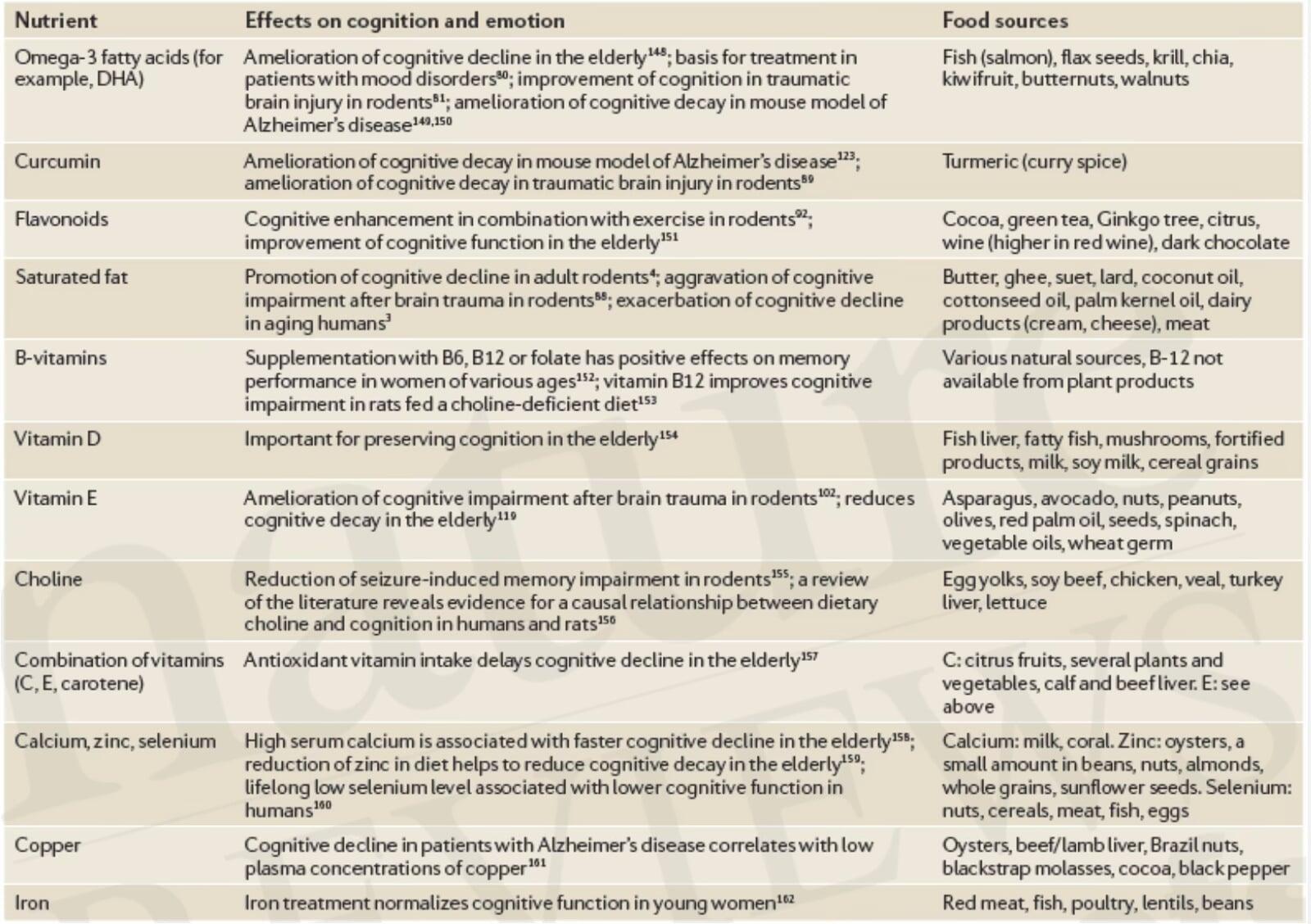
Figure 14: A schematic model of the effect of DHA upon neuronal survival. DHA is provided from astroglia incorporated into neurons and promotes PS accumulation by serving as the preferred substrate for PS biosynthesis. Membrane concentration of PS facilitates Akt translocation through interaction with basic residues in the PH domain, resulting in efficient phosphorylation and activation of Akt and suppressing caspase-3 activation and cell death. This occurs especially under adverse conditions where PIP3 generation is limited. DPA, replacing DHA in n-3 fatty acid deficiency, is not as effective as DHA in promoting PS accumulation and Akt translocation and is consequently less effective in supporting cell survival. DHA = docosahexaenoic acid; DPA = docosapentaenoic acid’ PIP3=" phosphatidylinositol" (3,4,5)-triphosphate; PS = phosphatidylserine; PC = phosphatidylcholine; PE = phosphatidylethanolamine
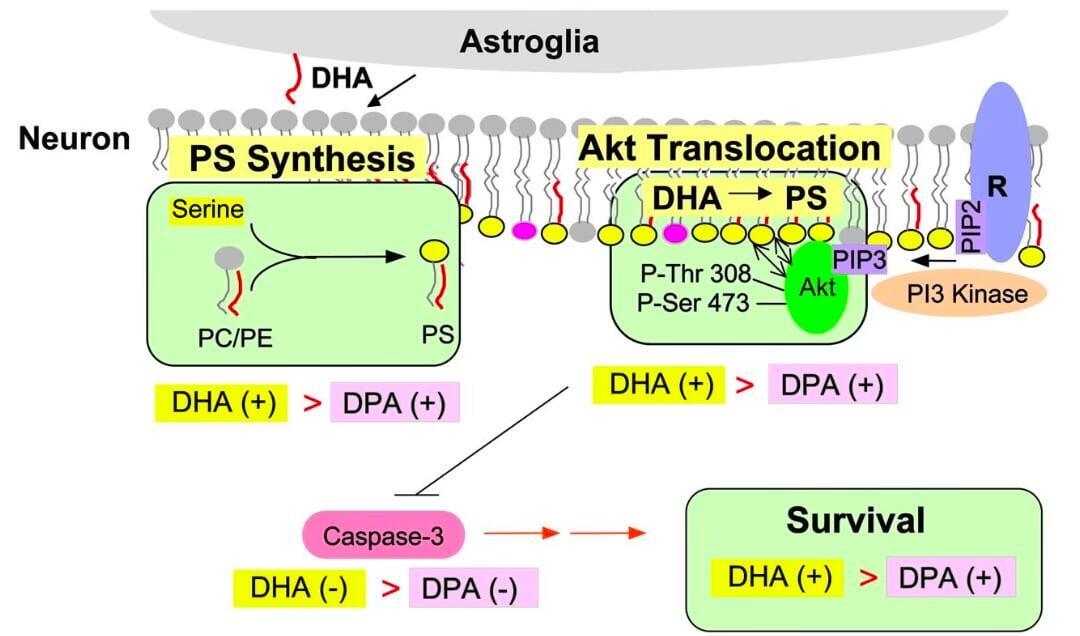
Beyond the understanding that 3-PUFAs play a critical role in membrane integrity, which would be seen as a factor in neurotransmission and neuroplasticity, is the finding that phospholipids containing high amounts of polyunsaturated fatty acids catalyse reactions which have been shown to hyperpolarise the reactive oxygen species plasma membrane and visual response. (194) This can be seen as a direct effect of 3-PUFAs upon neuroplasticity.
- To complement the salutary effects of exercise upon neuroplasticity as described above, a trial with experimental rats found that animals receiving 1.25% DHA for 12 days demonstrated significantly enhanced spatial learning effects as well as elevated levels of the neuroprotective BDNF. Levels of the signalling proteins cyclic AMP-response element (CREB_, Akt, CaMKII and synapsin I were increased as well, accompanied by the reduction of hippocampal oxidized protein levels. Clearly, DHA enhanced the effects of cognition and BDNF-related synaptic plasticity. (195)
- Conversely, diets high in saturated fats decreased the level of BDNF to the extent of compromising neuroplasticity and cognitive function. But if such high fat diets were supplemented with vitamin E, oxidative damage was dramatically reduced accompanied by normalised levels of BDNF, synapsin I, and CREB. (196)
- Reductions of BDNF, neuronal plasticity, and learning were confirmed in a second trial of rats put on a high-fat, refined sugar diet. (197)
- Even if normal diets were deficient in 3-PUFAs (in this case α-linolenic acid), both brain DHA and nerve growth factor levels in experimental rats fell to half of those seen in the control groups. Both were restored with the resumption of normal diet. (198)
- Age-dependent impairments in long-term potentiation, reflected by decreased transmitter release in the hippocampus of aged rats, have been proposed to be the product of increased membrane rigidity. Dietary supplementation of aged rats with omega-3 fatty acids restored the concentrations of both docosahexaenoic acid and arachidonic acid as two primary PUFAs in neuronal membranes. Eight weeks of the omega-3 fatty acids reversed the age-related impairments in long-term potentiation and the release of glutamate transmitter. Thus a link between membrane rigidity, neuroplasticity, and dietary manipulation was established. (199)
Botanicals
A subcategory of dietary additions to be considered as factors affecting neuroplasticity are the polyphenols, such as phenolic acids, stilbenes, lignans, flavonols, and anthocyanins. Some 8,000 compounds of these possess antioxidant properties and have been cited for reducing risks of neurodegenerative diseases and age-related cognitive decline as well as oxidative stress.
Polyphenols have been proposed to exert neuroprotective, neuroplastic, neurogenic, and anti-inflammatory effects. (200) A combination of studies from animal models have suggested that long-term supplementation with flavonoids, in particular, has modulated synaptic plasticity through the activation of neuronal receptors, signalling proteins (kinases), and gene expression. Human clinical studies have suggested that flavonoids, can positively affect peripheral and cerebrovascular blood flow, an indirect method by which flavonoids could affect brain health and cognition.
These pathways are shown in the schematic in Figure 15: (201)
Figure 15: Mechanisms underlying the effective dietary flavonoids on memory and learning. Circulating flavonoid metabolites might indirectly affect brain function and cognitive performance by modulating nitric oxide dependent cerebrovascular function at the level of the cerebral endothelium crossing the Blood Brain Barrier (BBB). Some flavonoid metabolites may act centrally by modulating neuronal receptors (e.g. TrkB, NMDA), signalling kinases (Akt, ERK ½) and neurotrophins (BDNF) to changes in synaptic function. NMDAR = n-methyl-D-aspartate receptor; TrkB = Tropomyosin receptor kinase B; Akt = protein kinase B; PKA = phosphokinase A; ERK = extracellular signal-related kinase; CREB = camp responsive element binding; eNOS = endothelial nitric oxide synthase; nNOS = neuronal nitric oxide synthase; ARC = activity-related cytoskeletal protein.
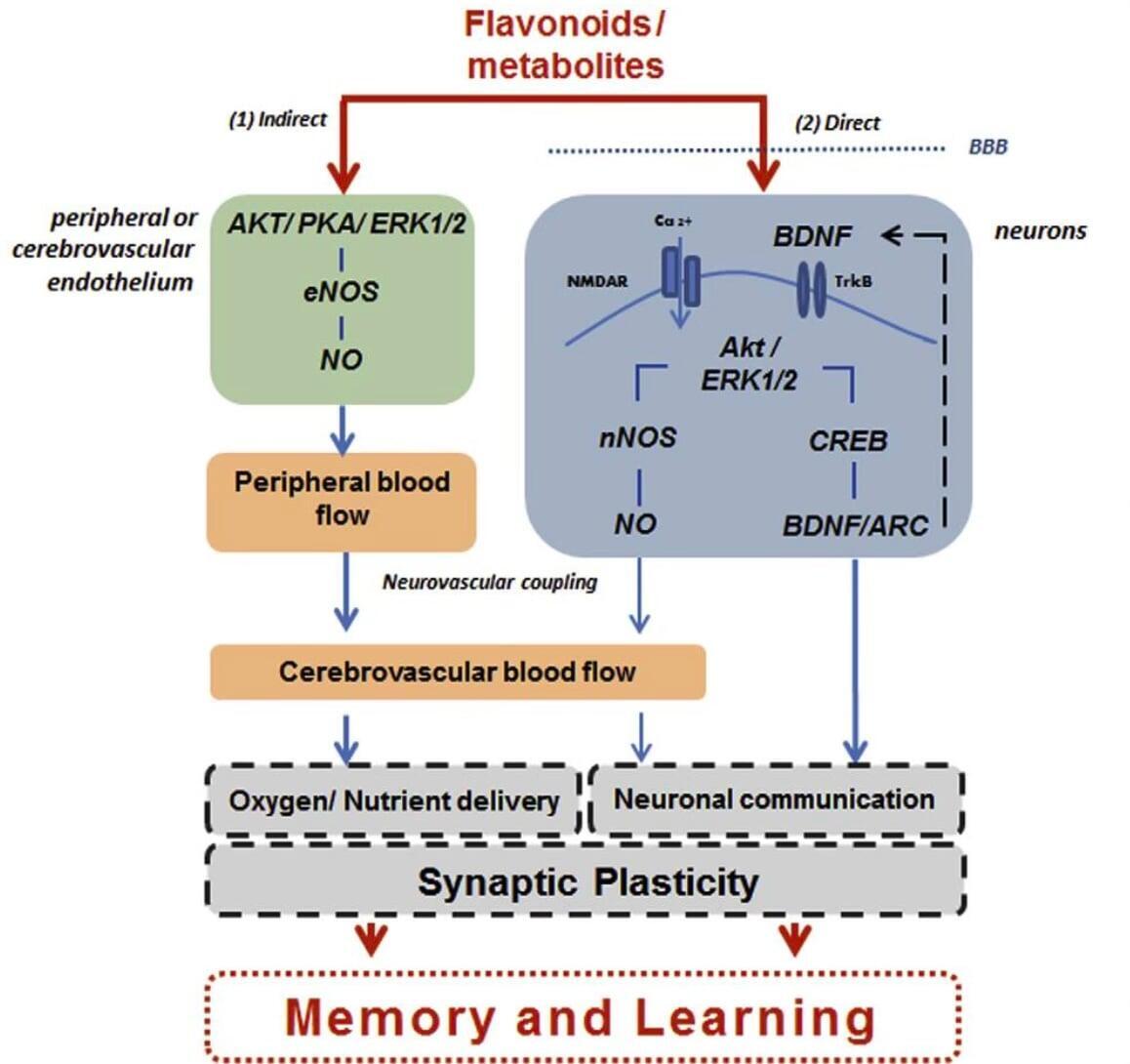
Effects of the most prominent botanicals are described below:
Curcumin:
- In mouse neural progenitor cells, curcumin activated extracellular signal-related kinases (ERKs) and p38 kinases, cellular signal transduction pathways known to be involved in the regulation of neuronal plasticity and stress responses. Inhibition of ERKs and p38 kinases effectively blocked the mitogenic effect of curcumin in these cells. (202)
- In rats subjected to traumatic brain injury, dietary supplementation with a curcumin derivative counteracted a multiplicity of effects of the injury, restoring parameters of membrane homeostasis and thus demonstrating an upregulation of neural repair and neuroplasticity. (203)
- The cerebral arteries from aging rats as well as endothelial cells showed that curcumin promoted eNOS and AMP phosphorylation, reducing superoxide anion production and attenuating aging-related cerebrovascular dysfunction. (204)
- Age-related loss of hippocampal synapse input specificity of long-term potentiation in mice was reversed by curcumin, re-establishing NMDA receptor dependence of induction. It also modulated hippocampal redox status by reducing age-related increases of the oxidative thiobarbituric acid-reactive substance concentration and raising depressed levels of glutathione. (205)
- Healthy adults aged 60-85 participating in a randomised, double-blind, placebo-controlled trial showed that working memory and mood (general fatigue, change in state calmness, contentedness) were significantly improved with a curcumin supplement taken either with a single dose or over a 4-week period. (206)
Green tea:
- The neurotoxicity of aluminium chloride injections into the brains of experimental rats, seen by changes in behaviour and antioxidant levels was reversed by the administration of green tea extracts. The authors suggested that the actions of (-) epigallocetachin gallate and (-) epicatechin, two compounds in abundance in green tea, improved mitochondrial and cholinergic synaptic functions. (207)
- Cultured cells which express TrkB (a high affinity receptor for BDNF), displayed the potentiation of the neurogenic action of BDNF attributed to epigallocatechin-3-gallate (EGCG), an active ingredient of green tea. This was accomplished by binding of the green tea to the cell surface-associated 67 kDa laminin receptor. (208)
- The mouse hippocampus displayed an enhanced response to high-frequency stimulation-evoked long-term potentiation when it was exposed to EGCG, again indicating the promotion of neuronal plasticity by this compound. (209)
- Experimental rats administered EGCG for 26 weeks compared to controls displayed an improved reference and working memory in a radial maze, in addition to reduced plasma concentrations of lipid peroxides and enhanced plasma ferric-reducing anti-oxidation power. Lower hippocampus reactive oxygen species concentrations were also present in the EGCG-fed animals. (210)
- The intake of catechins as a component of green tea, in addition to other polyphenols, displayed a positive association in 2,574 middle-aged adults with better language and verbal memory, but not with executive functioning, measured 13 years later. (211)
Resveratrol:
- Administration of resveratrol to mice subjected to a forced swim test and tail suspension test resulted in reduced immobility times while elevating BDNF and ERK phosphorylation levels in the prefrontal cortex and hippocampus. These antidepressant activities resembled those seen with the clinical antidepressant fluoxetine. The targets thus appeared to be the hypothalamic-pituitary-adrenal axis, BDNF, and ERK phosphorylation expression in the brain region. (212)
- A trial of rats subjected to chronic unpredictable mild stress for 5 weeks to induce depressive-like behaviour showed that resveratrol treatments for 5 weeks significantly reversed those behaviour abnormalities (reduced sucrose preference, increased immobility time and decreased locomotor activity). At the same time the BDNF levels that had been depressed in the hippocampus and amygdala accompanied by decreased phorphorylations of ERK, cAMP, and CREB were all reversed by resveratrol, mimicking the effects of the established antidepressant drug desipramine. (213) Highly congruent results involving spatial learning memory and BDNF levels with the addition of c-fos expression in the rat hippocampus and amygdala were obtained elsewhere. (214)
- Healthy older adults undergoing 26 weeks of resveratrol intake displayed a superior retention of words over 30 minutes compared with placebo, as well as significant increases of functional connectivity between the left posterior hippocampus and the medial prefrontal cortex as measured by fMRI. (215)
Conclusions
Functional neurology represents an overhaul of the early concepts of the capacity of neurons to integrate and then fire, (216) followed by a period of hyperpolarisation in which neurons became resistant to further stimuli. The updated concept of functional neurology represents the neuron integrated into its environment and therefore susceptible to modulations of its signalling capacity by a vast array of external factors.
These agents of change include both electrical and chemical phenomena triggered by such external interventions as rehabilitation, manual muscle therapy, acupuncture, biofeedback, aromatherapy, yoga, cognitive exercises, eye muscle exercises, mediation, exercise, diet, and botanical nutritional supplements. A significant body of literature has shown that all these measures offer the promise of adaptability and regeneration of elements of the nervous system in specific instances, perhaps to become more generalised with the completion further research.
In terms of aging and neurodegenerative diseases in particular, healthcare practices involving modalities that could be considered to be applications of functional neurology offer the possibility of retarding (and even reversing in certain instances) the progress of these undesirable conditions.
At the very least, the research studies summarised in this communication need to be duly admitted into the pantheon of evidence-based medicine, such that their application in the doctor’s office and healthcare systems in general may become more widely recognised as viable alternatives to current practices.
Author note
All images are retrieved from open-source materials publicly available by www. searching
References
1. Palmer DD. The Chiropractor's Adjuster: The Text-Book of the Science, Art and Philosophy of Chiropractic. Portland, OR: Portland Printing House; 1910.
2. Pascual-Leone A, Amedi A, Fregni F, Merabet LB. The plastic human brain cortex. Annu Rev Neurosci. 2005;28:377-401.
3. Conditions Treated with Functional Neurology. Functional Neurology Society.
4. Behrman S, Ebmeier K. Can exercise prevent cognitive decline? The Practitioner. 2014;258:17-21, 2-3.
5. Barnes JN. Exercise, cognitive function, and aging. Adv Physiol Educ. 2015;39:55-62.
6. Beck RW. Functional Neurology for Practitioners of Manual Medicine, 2nd Edition. Edinburgh: Churchill Livingstone; 2011.
7. Membrane potential and relativ. 3food.
8. Diamond MC, Krech D, Rosenzweig MR. The Effects of an Enriched Environment on the Histology of the Rat Cerebral Cortex. J Comp Neurol. 1964;123:111-20.
9. Odgen R, Franz S. On cerebral motor control: The recovery from experimentally produced hemiplegia. Psychol Health. 1917;1:33-49.
10. Franz SI, Scheetz ME, Wilson AAI. The possibility of recovery of motor function in long-standing hemiplegia. JAMA. 1915;65:2150-4.
11. Franz SI. The functions of the cerebrum. Psych Bull. 1916;13:149-73.
12. Neuropasticity and repair in the central nervous system: Implications for health care. WHO Offset Publ. 1983;73:1-56.
13. Lenn NJ. Neuroplasticity and the developing brain: implications for therapy. Pediatr Neurosci. 1987;13:176-83.
14. Carrick FR, Oggero E, Pagnacco G, Wright CH, Machado C, Estrada G, et al. Eye-movement training results in changes in qEEG and NIH Stroke Scale in subjects suffering from acute Middle Cerebral Artery Ischemic Stroke: A Randomized Control Trial. Front Neurol. 2016;7:3.
15. Synaptic Plasticity. Boundless Biology: Boundless.com.
16. Liu CZ, Kong J, Wang K. Acupuncture Therapies and Neuroplasticity. Neural Plast. 2017;2017:6178505.
17. Carrick FR. Changes in brain function after manipulation of the cervical spine. J Manipulative Physiol Ther. 1997;20:529-45.
18. Woollett K, Maguire EA. Acquiring "the Knowledge" of London's layout drives structural brain changes. Curr Biol. 2011;21:2109-14.
19. Maguire EA, Gadian DG, Johnsrude IS, Good CD, Ashburner J, Frackowiak RS, et al. Navigation-related structural change in the hippocampi of taxi drivers. Proc Natl Acad Sci U S A. 2000;97:4398-403.
20. Pelletier R, Higgins J, Bourbonnais D. Is neuroplasticity in the central nervous system the missing link to our understanding of chronic musculoskeletal disorders? BMC Musculoskelet Disord. 2015;16:25.
21. Altman J. Are new neurons formed in the brains of adult mammals? Science. 1962;135:1127-8.
22. Altman J, Das GD. Post-natal origin of microneurones in the rat brain. Nature. 1965;207:953-6.
23. Reynolds BA, Weiss S. Generation of neurons and astrocytes from isolated cells of the adult mammalian central nervous system. Science. 1992;255:1707-10.
24. Lois C, Alvarez-Buylla A. Long-distance neuronal migration in the adult mammalian brain. Science. 1994;264:1145-8.
25. Ernst A, Alkass K, Bernard S, Salehpour M, Perl S, Tisdale J, et al. Neurogenesis in the striatum of the adult human brain. Cell. 2014;156:1072-83.
26. Lois C, Kelsch W. Adult neurogenesis and its promise as a hope for brain repair. Front Neurosci. 2014;8:165.
27. Kelsch W, Mosley CP, Lin CW, Lois C. Distinct mammalian precursors are committed to generate neurons with defined dendritic projection patterns. PLoS Biol. 2007;5:e300.
28. Merkle FT, Mirzadeh Z, Alvarez-Buylla A. Mosaic organization of neural stem cells in the adult brain. Science. 2007;317:381-4.
29. Eriksson PS, Perfilieva E, Bjork-Eriksson T, Alborn AM, Nordborg C, Peterson DA, et al. Neurogenesis in the adult human hippocampus. Nat Med. 1998;4:1313-7.
30. Stevens CF. The neuron. Sci Am. 1979;241:54-65.
31. Overview of neuron structure and function. Khan Academy.
32. Koolman J, Klaus-Heinrich R. Color Atlas of Biochemistry. Stuttgart - New York: Thieme; 1996.
33. Olsen RW, DeLorey TM. GABA receptor physiology and pharmacology. Philadelphia, PA: Lippinott-Raven; 1999.
34. Benarroch EE. GABAB receptors: structure, functions, and clinical implications. Neurology. 2012;78:578-84.
35. Enna SJ, Bowery NG. The GABA Receptors, 2nd edition. Totowa, NJ: Humana; 1997.
36. Johnson GAR. Molecular biology, pharmacology, and physiology of GABAc receptors. Totowa, NJ: Humana; 1997.
37. Polenzani L, Woodward RM, Miledi R. Expression of mammalian gamma-aminobutyric acid receptors with distinct pharmacology, in Xenopus oocytes. Proc Natl Acad Sci U S A. 1991;88:4318-22.
38. Dong CJ, Werblin FS. Dopamine modulation of GABAC receptor function in an isolated retinal neuron. J Neurophysiol. 1994;71:1258-60.
39. Wellis DP, Werblin FS. Dopamine modulates GABAc receptors mediating inhibition of calcium entry into and transmitter release from bipolar cell terminals in tiger salamander retina. J Neurosci. 1995;15:4748-61.
40. Tsien JZ. Building a brainier mouse. Sci Am. 2000;282:62-8.
41. Furukawa H, Singh SK, Mancusso R, Gouaux E. Subunit arrangement and function in NMDA receptors. Nature. 2005;438:185-92.
42. Kleckner NW, Dingledine R. Requirement for glycine in activation of NMDA-receptors expressed in Xenopus oocytes. Science. 1988;241:835-7.
43. Purves D, Augustine GJ, Fitzpatric D, Hall WC, LaMantia AS, McNamara JO, White LE. Neurosience, 4th edition. Sunderland, MA: Sinauer Associates; 2008, pp. 129-131.
44. Dingledine R, Borges K, Bowie D, Traynelis SF. The glutamate receptor ion channels. Pharmacol Rev. 1999;51:7-61.
45. Paoletti P, Neyton J. NMDA receptor subunits: function and pharmacology. Curr Opin Pharmacol. 2007;7:39-47.
46. Li S, Jin M, Koeglsperger T, Shepardson NE, Shankar GM, Selkoe DJ. Soluble Abeta oligomers inhibit long-term potentiation through a mechanism involving excessive activation of extrasynaptic NR2B-containing NMDA receptors. J Neurosci. 2011;31:6627-38.
47. Parsons MP, Raymond LA. Extrasynaptic NMDA receptor involvement in central nervous system disorders. Neuron. 2014;82:279-93.
48. Schultz W. Multiple dopamine functions at different time courses. Annu Rev Neurosci. 2007;30:259-88.
49. Perrin RN. Lymphatic drainage of the neuraxis in chronic fatigue syndrome: a hypothetical model for the cranial rhythmic impulse. J Am Osteopath Assoc. 2007;107:218-24.
50. Callier S, Snapyan M, Le Crom S, Prou D, Vincent JD, Vernier P. Evolution and cell biology of dopamine receptors in vertebrates. Biol Cell. 2003;95:489-502.
51. Lee SP, So CH, Rashid AJ, Varghese G, Cheng R, Lanca AJ, et al. Dopamine D1 and D2 receptor Co-activation generates a novel phospholipase C-mediated calcium signal. J Biol Chem. 2004;279:35671-8.
52. Hiroi N, Martin AB, Grande C, Alberti I, Rivera A, Moratalla R. Molecular dissection of dopamine receptor signaling. J Chem Neuroanat. 2002;23:237-42.
53. Hasbi A, O'Dowd BF, George SR. Heteromerization of dopamine D2 receptors with dopamine D1 or D5 receptors generates intracellular calcium signaling by different mechanisms. Curr Opin Pharmacol. 2010;10:93-9.
54. Rhodes JS, Garland T, Jr., Gammie SC. Patterns of brain activity associated with variation in voluntary wheel-running behavior. Behav Neurosci. 2003;117:1243-56.
55. Gerfen CR, Engber TM, Mahan LC, Susel Z, Chase TN, Monsma FJ, Jr., et al. D1 and D2 dopamine receptor-regulated gene expression of striatonigral and striatopallidal neurons. Science. 1990;250:1429-32.
56. Steiner H, Gerfen CR. Dynorphin regulates D1 dopamine receptor-mediated responses in the striatum: relative contributions of pre- and postsynaptic mechanisms in dorsal and ventral striatum demonstrated by altered immediate-early gene induction. J Comp Neurol. 1996;376:530-41.
57. Le Moine C, Normand E, Guitteny AF, Fouque B, Teoule R, Bloch B. Dopamine receptor gene expression by enkephalin neurons in rat forebrain. Proc Natl Acad Sci U S A. 1990;87:230-4.
58. Korotkova TM, Brown RE, Sergeeva OA, Ponomarenko AA, Haas HL. Effects of arousal- and feeding-related neuropeptides on dopaminergic and GABAergic neurons in the ventral tegmental area of the rat. Eur J Neurosci. 2006;23:2677-85.
59. Wise RA. Dopamine, learning and motivation. Nat Rev Neurosci. 2004;5:483-94.
60. Jackson DM, Westlind-Danielsson A. Dopamine receptors: molecular biology, biochemistry and behavioural aspects. Pharmacol Ther. 1994;64:291-370.
61. Zhang J, Goodlett DR. Proteomic approach to studying Parkinson's disease. Mol Neurobiol. 2004;29:271-88.
62. Levy F. What do dopamine transporter and catechol-o-methyltransferase tell us about attention deficit–hyperactivity disorder? Pharmacogenomic implications. Aust N Z J Psychiatry. 2007;41:10-6.
63. Di Chiara G. The role of dopamine in drug abuse viewed from the perspective of its role in motivation. Drug Alcohol Depend. 1995;38:95-137.
64. Bove AA, Dewey JD, Tyce GM. Increased conjugated dopamine in plasma after exercise training. J Lab Clin Med. 1984;104:77-85.
65. Hartling OJ, Kelbaek H, Gjorup T, Nielsen MD, Trap-Jensen J. Plasma concentrations of adrenaline, noradrenaline and dopamine during forearm dynamic exercise. Clin Physiol. 1989;9:399-404.
66. Peronnet F, Cleroux J, Perrault H, Thibault G, Cousineau D, de Champlain J, et al. Plasma norepinephrine, epinephrine, and dopamine beta-hydroxylase activity during exercise in man. Med Sci Sports Exerc. 1985;17:683-8.
67. Robertson S. Role of dopamine in pain. 2016.
68. Glatz K, Mossner R, Heils A, Lesch KP. Glucocorticoid-regulated human serotonin transporter (5-HTT) expression is modulated by the 5-HTT gene-promotor-linked polymorphic region. J Neurochem. 2003;86:1072-8.
69. Phelps J. Chapter 4: Connecting anxiety and depression via the serotonin transporter gene. PsychEducationorg. 2000-2016.
70. Young SN. How to increase serotonin in the human brain without drugs. J Psychiatry Neurosci. 2007;32:394.
71. Chanrion B, Mannoury la Cour C, Bertaso F, Lerner-Natoli M, Freissmuth M, Millan MJ, Bockaert J, Marin P. Physical interaction between the serotonin transporter and neuronal nitric oxide synthase underlies reciprocal modulation of their activity. Proc Natl Acad Sci U S A. 2007;104:8119-24.
72. Heisler LK, Jobst EE, Sutton GM, Zhou L, Borok E, Thornton-Jones Z, et al. Serotonin reciprocally regulates melanocortin neurons to modulate food intake. Neuron. 2006;51:239-49.
73. Zhou L, Sutton GM, Rochford JJ, Semple RK, Lam DD, Oksanen LJ, et al. Serotonin 2C receptor agonists improve type 2 diabetes via melanocortin-4 receptor signaling pathways. Cell Metab. 2007;6:398-405.
74. Inose H. Control of bone remodeling by nervous system. The role of serotonin in the regulation of bone metabolism. Clin Calcium. 2010;20:1850-956.
75. Byrne JH. Section 1: Cellular and Molecular Neurobiology. Introduction to Neurons and Neuronal Networks. Houston, TX: University of Texas Medical School Health Sciences Center; 1997.
76. Smith Y, Wichmann T, Factor SA, DeLong MR. Parkinson's disease therapeutics: new developments and challenges since the introduction of levodopa. Neuropsychopharmacology. 2012;37:213-46.
77. Galvan A, Wichmann T. Pathophysiology of parkinsonism. Clin Neurophysiol. 2008;119:1459-74.
78. Geschwind N, Levitsky W. Human brain: left-right asymmetries in temporal speech region. Science. 1968;161:186-7.
79. Steinmetz H, Huang YX. Two-dimensional mapping of brain surface anatomy. AJNR Am J Neuroradiol. 1991;12:997-1000.
80. Davidson RJ, Hugdahl K. Brain asymmetry. Cambridge, MA: MIT Press; 1996.
81. Morton LL, Allen JD, Williams NH. Hemisphericity and information processing in North American Native (Ojibwa) and non-native adolescents. Int J Neurosci. 1994;75:189-202.
82. Tiller SG, Persinger MA. Elevated incidence of a sensed presence and sexual arousal during partial sensory deprivation and sensitivity to hypnosis: implications for hemisphericity and gender differences. Percept Mot Skills. 1994;79:1527-31.
83. Lazure CL, Persinger MA. Right hemisphericity and low self-esteem in high school students: a replication. Percept Mot Skills. 1992;75:1058.
84. Barnhart RC, Davenport MJ, Epps SB, Nordquist VM. Developmental coordination disorder. Phys Ther. 2003;83:722-31.
85. Neurology PC. Functional Neurology Rehabilitation. Portland, ME.
86. Kerkhoff G, Keller I, Ritter V, Marquardt C. Repetitive optokinetic stimulation induces lasting recovery from visual neglect. Restor Neurol Neurosci. 2006;24:357-69.
87. Pavlou M, Quinn C, Murray K, Spyridakou C, Faldon M, Bronstein AM. The effect of repeated visual motion stimuli on visual dependence and postural control in normal subjects. Gait Posture. 2011;33:113-8.
88. Pavlou M, Bronstein AM, Davies RA. Randomized trial of supervised versus unsupervised optokinetic exercise in persons with peripheral vestibular disorders. Neurorehabil Neural Repair. 2013;27:208-18.
89. Park IS, Lee NJ, Kim TY, Park JH, Won YM, Jung YJ, et al. Volumetric analysis of cerebellum in short-track speed skating players. Cerebellum. 2012;11:925-30.
90. Drijkoningen D, Caeyenberghs K, Leunissen I, Vander Linden C, Leemans A, Sunaert S, Duysens J, Swinnen SP. Training-induced improvements in postural control are accompanied by alterations in cerebellar white matter in brain injured patients. Neuroimage Clin. 2015;7:240-51.
91. Bastian A, Keller JL. A home balance exercise program improves walking in people with cerebellar ataxia. Neurorehabil Neural Repair. 2014;28:770-8.
92. Meier J, Topka MS, Hanggi J. Differences in cortical representation and structural connectivity of hands and feet between professional Handball players and ballet dancers. Neural Plast. 2016;2016:6817397.
93. Beurskens R, Steinberg F, Antoniewicz F, Wolff W, Granacher U. Neural correlates of dual-task walking: Effects of cognitive versus motor interference in young adults. Neural Plast. 2016;2016:8032180.
94. Thomas R, Beck MM, Lind RR, Korsgaard Johnsen L, Geertsen SS, Christiansen L, et al. Acute Exercise and Motor Memory Consolidation: The Role of Exercise Timing. Neural Plast. 2016;2016:6205452.
95. Niemann C, Godde B, Voelcker-Rehage C. Senior Dance Experience, Cognitive Performance, and Brain Volume in Older Women. Neural Plast. 2016;2016:9837321.
96. Ricci NA, Aratani MC, Doná F, Macedo C, Caovilla HH, Ganança FF. A systematic review about the effects of the vestibular rehabilitation in middle-age and older adults. Brazilian Journal of Physical Therapy. 2010;14:361-71.
97. Tsukamoto HF, Costa Vde S, Silva RAJ, Pelosi GG, Marchiori LL, Vaz CR, et al. Effectiveness of a Vestibular Rehabilitation Protocol to Improve the Health-Related Quality of Life and Postural Balance in Patients with Vertigo. Int Arch Otorhinolaryngol. 2015;19:238-47.
98. Bergeron M, Lortie CL, Guitton MJ. Use of Virtual Reality Tools for Vestibular Disorders Rehabilitation: A Comprehensive Analysis.Adv Med. 2015;2015:916735.
99. Lacour M, Bernard-Demanze L. Interaction between vestibular compensation mechanisms and vestibular rehabilitation therapy: 10 Recommendations for Optimal Functional Recovery. Front Neurol. 2014;5:285.
100. Dawson G. Early behavioral intervention, brain plasticity, and the prevention of autism spectrum disorder. Dev Psychopathol. 2008;20:775-803.
101. Golestani N, Paus T, Zatorre RJ. Anatomical correlates of learning novel speech sounds. Neuron. 2002;35:997-1010.
102. Tallal P. Language learning disabilities: Integrating research approaches. Curr Dir Psychol Sci. 2003;12:206-11.
103. Eden GF, Jones KM, Cappell K, Gareau L, Wood FB, Zeffiro TA, et al. Neural changes following remediation in adult developmental dyslexia. Neuron. 2004;44:411-22.
104. Mishra J, Merzenich MM, Sagar R. Accessible online neuroplasticity-targeted training for children with ADHD. Child Adolesc Psychiatry Ment Health. 2013;7:38.
105. Buch E, Weber C, Cohen LG, Braun C, Dimyan MA, Ard T, et al. Think to move: a neuromagnetic brain-computer interface (BCI) system for chronic stroke. Stroke. 2008;39:910-7.
106. Korr IM. Preface in Neurobiologic Mechanisms in Manipulative Therapy. New York: Plenum; 1978, pp. xv-xvii.
107. Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). I. Effects on dorsal horn convergent neurones in the rat. Pain. 1979;6:283-304.
108. Sato A, Swenson RS. Sympathetic nervous system response to mechanical stress of the spinal column in rats. J Manipulative Physiol Ther. 1984;7:141-7.
109. Welch A, Boone R. Sympathetic and parasympathetic responses to specific diversified adjustments to chiropractic vertebral subluxations of the cervical and thoracic spine. J Chiropr Med. 2008;7:86-93.
110. Zane T. A review of craniosacral therapy: Science, fads, and applied behavior analysis. The Current Repertoire. Cambridge, MA: Cambridge Center for Behavioral Studies, Inc. ; 2011.
111. Jakel A, von Hauenschild P. A systematic review to evaluate the clinical benefits of craniosacral therapy. Complement Ther Med. 2012;20:456-65.
112. Girsberger W, Banziger U, Lingg G, Lothaller H, Endler PC. Heart rate variability and the influence of craniosacral therapy on autonomous nervous system regulation in persons with subjective discomforts: a pilot study. J Integr Med. 2014;12:156-61.
113. Kratz SV, Kerr J, Porter L. The use of CranioSacral therapy for Autism Spectrum Disorders: Benefits from the viewpoints of parents, clients, and therapists. J Bodyw Mov Ther. 2017;21:19-29.
114. Haller H, Lauche R, Cramer H, Rampp T, Saha FJ, Ostermann T, et al. Craniosacral therapy for the treatment of chronic neck pain: A randomized sham-controlled trial. Clin J Pain. 2016;32:441-9.
115. Castro-Sanchez AM, Lara-Palomo IC, Mataran-Penarrocha GA, Saavedra-Hernandez M, Perez-Marmol JM, Aguilar-Ferrandiz ME. Benefits of Craniosacral therapy in patients with chronic low back pain: A randomized controlled trial. J Altern Complement Med. 2016;22:650-7.
116. Arnadottir TS, Sigurdardottir AK. Is craniosacral therapy effective for migraine? Tested with HIT-6 Questionnaire. Complement Ther Clin Pract. 2013;19:11-4.
117. Mataran-Penarrocha GA, Castro-Sanchez AM, Garcia GC, Moreno-Lorenzo C, Carreno TP, Zafra MD. Influence of craniosacral therapy on anxiety, depression and quality of life in patients with fibromyalgia. Evid Based Complement Alternat Med. 2011;2011:178769.
118. Ning Y, Li K, Fu C, Ren Y, Zhang Y, Liu H, et al. Enhanced functional connectivity between the bilateral primary motor cortices after acupuncture at Yanglingquan (GB34) in right-hemispheric subcortical stroke patients: A resting-state fMRI study. Front Hum Neurosci. 2017;11:178.
119. Liu W, Wu J, Huang J, Zhuo P, Lin Y, Wang L, et al. Electroacupuncture Regulates Hippocampal Synaptic Plasticity via miR-134- Mediated LIMK1 Function in Rats with Ischemic Stroke. Neural Plast. 2017;2017:9545646.
120. Mo YP, Yao HJ, Lv W, Song LY, Song HT, Yuan XC, et al. Effects of electroacupuncture at Governor Vessel acupoints on Neurotrophin-3 in rats with experimental spinal cord Injury. Neural Plast. 2016;2016:2371875.
121. Yang JW, Ye Y, Wang XR, Li F, Xiao LY, Shi GX, et al. Acupuncture attenuates renal sympathetic activity and blood pressure via Beta-Adrenergic receptors in spontaneously hypertensive rats. Neural Plast. 2017;2017:8696402.
122. Shao XM, Sun J, Jiang YL, Liu BY, Shen Z, Fang F, et al. Inhibition of the cAMP/PKA/CREB pathway contributes to the analgesic effects of electroacupuncture in the Anterior Cingulate cortex in a rat pain memory model. Neural Plast. 2016;2016:5320641.
123. Sun N, Zou X, Shi J, Liu X, Li L, Zhao L. Electroacupuncture regulates NMDA receptor NR1 subunit expression via PI3-K pathway in a rat model of cerebral ischemia-reperfusion. Brain Res. 2005;1064:98-107.
124. Shibata K, Watanabe T, Sasaki Y, Kawato M. Perceptual learning incepted by decoded fMRI neurofeedback without stimulus presentation. Science. 2011;334:1413-5.
125. Scharnowski F, Hutton C, Josephs O, Weiskopf N, Rees G. Improving visual perception through neurofeedback. J Neurosci. 2012;32:17830-41.
126. Seitz AR. Cognitive neuroscience: targeting neuroplasticity with neural decoding and biofeedback. Curr Biol. 2013;23:R210-2.
127. Alvarez J, Meyer FL, Granoff DL, Lundy A. The effect of EEG biofeedback on reducing postcancer cognitive impairment. Integr Cancer Ther. 2013;12:475-87.
128. Ghaziri J, Tucholka A, Larue V, Blanchette-Sylvestre M, Reyburn G, Gilbert G, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-72.
129. Woodford H, Price C. EMG biofeedback for the recovery of motor function after stroke. The Cochrane database of systematic reviews. 2007:CD004585.
130. Lorig TS, Schwartz GE. Brain and odor: I. Alteration of human EEG by odor administration. Psychobiology. 1988.
131. Brauchli P, Ruegg PB, Etzweiler F, Zeier H. Electrocortical and autonomic alteration by administration of a pleasant and an unpleasant odor. Chem Senses. 1995;20:505-15.
132. Haze S, Sakai K, Gozu Y. Effects of fragrance inhalation on sympathetic activity in normal adults. Jpn J Pharmacol. 2002;90:247-53.
133. Manley CH. Psychophysiological effect of odor. Crit Rev Food Sci Nutr. 1993;33:57-62.
134. Heuberger E, Hongratanaworakit T, Bohm C, Weber R, Buchbauer G. Effects of chiral fragrances on human autonomic nervous system parameters and self-evaluation. Chem Senses. 2001;26:281-92.
135. Cho MY, Min ES, Hur MH, Lee MS. Effects of aromatherapy on the anxiety, vital signs, and sleep quality of percutaneous coronary intervention patients in intensive care units. Evid Based Complement Alternat Med. 2013;2013:381381.
136. Functional Neuro--A Different Bodywork Approach. Integration Massage,2013.
137. Diego MA, Field T. Moderate pressure massage elicits a parasympathetic nervous system response. Int J Neurosci. 2009;119:630-8.
138. Bazzichi L, Dini M, Rossi A, Corbianco S, Giovannoni E, Consensi A, et al. A combination therapy of massage and stretching increases parasympathetic nervous activity and improves joint mobility in patients affected by fibromyalgia. Health (N Y). 2010;2:919.
139. Guan L, Collet JP, Yuskiv N, Skippen P, Brant R, Kissoon N. The effect of massage therapy on autonomic activity in critically ill children. Evid Based Complement Alternat Med. 2014;2014:656750.
140. Lee YH, Park BN, Kim SH. The effects of heat and massage application on autonomic nervous system. Yonsei Med J. 2011;52:982-9.
141. Hadlock T, Lindsay R, Edwards C, Smitson C, Weinberg J, Knox C, et al. The effect of electrical and mechanical stimulation on the regenerating rodent facial nerve. Laryngoscope. 2010;120:1094-102.
142. Skouras E, Ozsoy U, Sarikcioglu L, Angelov DN. Intrinsic and therapeutic factors determining the recovery of motor function after peripheral nerve transection. Ann Anat. 2011;193:286-303.
143. Naveen GH, Thirthalli J, Rao MG, Varambally S, Christopher R, Gangadhar BN. Positive therapeutic and neurotropic effects of yoga in depression: A comparative study. Indian J Psychiatry. 2013;55:S400-4.
144. Froeliger B, Garland EL, McClernon FJ. Yoga meditation practitioners exhibit greater gray matter volume and fewer reported cognitive failures: results of a preliminary voxel-based morphometric analysis. Evid Based Complement Alternat Med. 2012;2012:821307.
145. Villemure C, Ceko M, Cotton VA, Bushnell MC. Neuroprotective effects of yoga practice: age-, experience-, and frequency-dependent plasticity. Front Hum Neurosci. 2015;9:281.
146. Malhotra V, Singh S, Tandon OP, Madhu SV, Prasad A, Sharma SB. Effect of Yoga asanas on nerve conduction in type 2 diabetes. Indian J Physiol Pharmacol. 2002;46:298-306.
147. Balasubramanian S, Mintzer JE, Wahlquist AE. Induction of salivary nerve growth factor by Yogic breathing: a randomized controlled trial. Int Psychogeriatr. 2015;27:168-70.
148. Bergland C. Eight Habits that Improve Cognitive Function. Psychol Today2014.
149. Pfurtscheller G, Neuper C, Ramoser H, Muller-Gerking J. Visually guided motor imagery activates sensorimotor areas in humans.Neurosci Lett. 1999;269:153-6.
150. Hovington CL, Brouwer B. Guided motor imagery in healthy adults and stroke: does strategy matter? Neurorehabil Neural Repair. 2010;24:851-7.
151. Lee SE, Han Y, Park H. Neural Activations of Guided Imagery and Music in Negative Emotional Processing: A Functional MRI Study. J Music Ther. 2016;53:257-78.
152. Moseley GL. Using visual illusion to reduce at-level neuropathic pain in paraplegia. Pain. 2007;130:294-8. 153. MacIver K, Lloyd DM, Kelly S, Roberts N, Nurmikko T. Phantom limb pain, cortical reorganization and the therapeutic effect of mental imagery. Brain. 2008;131:2181-91.
154. Sebastiani L, Simoni A, Gemignani A, Ghelarducci B, Santarcangelo EL. Human hypnosis: autonomic and electroencephalographic correlates of a guided multimodal cognitive-emotional imagery. Neurosci Lett. 2003;338:41-4.
155. Ostberg O, Horie Y, Feng Y. On the merits of ancient Chinese eye acupressure practices. Appl Ergon. 1992;23:343-8.
156. Li SM, Kang MT, Peng XX, Li SY, Wang Y, Li L, et al. Efficacy of Chinese eye exercises on reducing accommodative lag in school-aged children: a randomized controlled trial. PLoS One. 2015;10:e0117552.
157. Horwood AM, Toor SS, Riddell PM. Change in convergence and accommodation after two weeks of eye exercises in typical young adults. J AAPOS. 2014;18:162-8.
158. Kim SD. Effects of yogic eye exercises on eye fatigue in undergraduate nursing students. J Phys Ther Sci. 2016;28:1813-5.
159. Di Noto P, Uta S, DeSouza JF. Eye exercises enhance accuracy and letter recognition, but not reaction time, in a modified rapid serial visual presentation task. PLoS One. 2013;8:e59244.
160. Rodriguez SL, Hopman WM, ten Hove MW. Eye exercises for treatment of idiopathic cranial nerve VII paresis: pilot study. Can J Neurol Sci. 2012;39:196-201.
161. Rawstron JA, Burley CD, Elder MJ. A systematic review of the applicability and efficacy of eye exercises. J Pediatr Ophthalmol Strabismus. 2005;42:82-8.
162. Wilson A. Mindfulness, Meditation and the Brain. Huffington Post; 2013.
163. Treadway MT, Lazar SW. Mediation and Neuroplasticity: Using Mindfulness to Change the Brain: Context Press.
164. Brefczynski-Lewis JA, Lutz A, Schaefer HS, Levinson DB, Davidson RJ. Neural correlates of attentional expertise in long-term meditation practitioners. Proc Natl Acad Sci U S A. 2007;104:11483-8.
165. Lutz A, Greischar LL, Rawlings NB, Ricard M, Davidson RJ. Long-term meditators self-induce high-amplitude gamma synchrony during mental practice. Proc Natl Acad Sci U S A. 2004;101:16369-73.
166. Lutz A, Brefczynski-Lewis J, Johnstone T, Davidson RJ. Regulation of the neural circuitry of emotion by compassion meditation: effects of meditative expertise. PLoS One. 2008;3:e1897.
167. Slagter HA, Lutz A, Greischar LL, Francis AD, Nieuwenhuis S, Davis JM, et al. Mental training affects distribution of limited brain resources. PLoS Biol. 2007;5:e138.
168. Holzel BK, Carmody J, Evans KC, Hoge EA, Dusek JA, Morgan L, et al. Stress reduction correlates with structural changes in the amygdala. Soc Cogn Affect Neurosci. 2010;5:11-7.
169. Luders E, Toga AW, Lepore N, Gaser C. The underlying anatomical correlates of long-term meditation: larger hippocampal and frontal volumes of gray matter. Neuroimage. 2009;45:672-8.
170. Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, et al. Meditation experience is associated with increased cortical thickness. Neuroreport. 2005;16:1893-7.
171. Vestergaard-Poulsen P, van Beek M, Skewes J, Bjarkam CR, Stubberup M, Bertelsen J, et al. Long-term meditation is associated with increased gray matter density in the brain stem. Neuroreport. 2009;20:170-4.
172. Tang YY, Lu Q, Fan M, Yang Y, Posner MI. Mechanisms of white matter changes induced by meditation. Proc Natl Acad Sci U S A. 2012;109:10570-4.
173. Tomporowski PD, Davis CL, Miller PH, Naglieri JA. Exercise and Children's Intelligence, Cognition, and Academic Achievement. Educ Psychol Rev. 2008;20:111-31.
174. Erickson KI, Raji CA, Lopez OL, Becker JT, Rosano C, Newman AB, et al. Physical activity predicts gray matter volume in late adulthood: the Cardiovascular Health Study. Neurology. 2010;75:1415-22.
175. Jacini WF, Cannonieri GC, Fernandes PT, Bonilha L, Cendes F, Li LM. Can exercise shape your brain? Cortical differences associated with judo practice. J Sci Med Sport. 2009;12:688-90.
176. Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A. 2011;108:3017-22.
177. Pereira AC, Huddleston DE, Brickman AM, Sosunov AA, Hen R, McKhann GM, et al. An in vivo correlate of exercise-induced neurogenesis in the adult dentate gyrus. Proc Natl Acad Sci U S A. 2007;104:5638-43.
178. Themanson JR, Pontifex MB, Hillman CH. Fitness and action monitoring: evidence for improved cognitive flexibility in young adults. Neuroscience. 2008;157:319-28.
179. Pontifex MB, Hillman CH, Polich J. Age, physical fitness, and attention: P3a and P3b. Psychophysiology. 2009;46:379-87.
180. Gomez-Pinilla F, Vaynman S, Ying Z. Brain-derived neurotrophic factor functions as a metabotrophin to mediate the effects of
exercise on cognition. Eur J Neurosci. 2008;28:2278-87.
181. Ding Q, Vaynman S, Akhavan M, Ying Z, Gomez-Pinilla F. Insulin-like growth factor I interfaces with brain-derived neurotrophic factor-mediated synaptic plasticity to modulate aspects of exercise-induced cognitive function. Neuroscience. 2006;140:823-33.
182. Fabel K, Fabel K, Tam B, Kaufer D, Baiker A, Simmons N, et al. VEGF is necessary for exercise-induced adult hippocampal neurogenesis. Eur J Neurosci. 2003;18:2803-12.
183. Gomez-Pinilla F, Hillman C. The influence of exercise on cognitive abilities. Compr Physiol. 2013;3:403-28.
184. Petzinger GM, Fisher BE, McEwen S, Beeler JA, Walsh JP, Jakowec MW. Exercise-enhanced neuroplasticity targeting motor and cognitive circuitry in Parkinson's disease. Lancet Neurol. 2013;12:716-26.
185. Stranahan AM, Khalil D, Gould E. Running induces widespread structural alterations in the hippocampus and entorhinal cortex. Hippocampus. 2007;17:1017-22.
186. Pysh JJ, Weiss GM. Exercise during development induces an increase in Purkinje cell dendritic tree size. Science. 1979;206:230-2.
187. Uswatte G, Taub E. Constraint-induced movement therapy: a method for harnessing neuroplasticity to treat motor disorders. Prog Brain Res. 2013;207:379-401.
188. Mark VW, Taub E, Morris DM. Neuroplasticity and constraint-induced movement therapy. Eura Medicophys. 2006;42:269-84.
189. Massie CL, Kantak SS, Narayanan P, Wittenberg GF. Timing of motor cortical stimulation during planar robotic training differentially impacts neuroplasticity in older adults. Clin Neurophysiol. 2015;126:1024-32.
190. Alsubiheen A, Petrofsky J, Daher N, Lohman E, Balbas E, Lee H. Tai Chi with mental imagery theory improves soleus H-reflex and nerve conduction velocity in patients with type 2 diabetes. Complement Ther Med. 2017;31:59-64.
191. Gomez-Pinilla F. Brain foods: the effects of nutrients on brain function. Nat Rev Neurosci. 2008;9:568-78.
192. Akbar M, Calderon F, Wen Z, Kim HY. Docosahexaenoic acid: a positive modulator of Akt signaling in neuronal survival. Proc Natl Acad Sci U S A. 2005;102:10858-63.
193. Kim H-Y. Docosahexaenoic acid: membrane modification and neurotrophic mechanisms. Oléagineux, Corps gras, Lipides. 2011;18:237-41.
194. Jump DB. The biochemistry of n-3 polyunsaturated fatty acids. J Biol Chem. 2002;277:8755-8.
195. Wu A, Ying Z, Gomez-Pinilla F. Docosahexaenoic acid dietary supplementation enhances the effects of exercise on synaptic plasticity and cognition. Neuroscience. 2008;155:751-9.
196. Wu A, Ying Z, Gomez-Pinilla F. The interplay between oxidative stress and brain-derived neurotrophic factor modulates the outcome of a saturated fat diet on synaptic plasticity and cognition. Eur J Neurosci. 2004;19:1699-707.
197. Molteni R, Barnard RJ, Ying Z, Roberts CK, Gomez-Pinilla F. A high-fat, refined sugar diet reduces hippocampal brain-derived neurotrophic factor, neuronal plasticity, and learning. Neuroscience. 2002;112:803-14.
198. Ikemoto A, Nitta A, Furukawa S, Ohishi M, Nakamura A, Fujii Y, et al. Dietary n-3 fatty acid deficiency decreases nerve growth factor content in rat hippocampus. Neurosci Lett. 2000;285:99-102.
199. McGahon BM, Martin DS, Horrobin DF, Lynch MA. Age-related changes in synaptic function: analysis of the effect of dietary supplementation with omega-3 fatty acids. Neuroscience. 1999;94:305-14.
200. Phillips C. Lifestyle Modulators of Neuroplasticity: How Physical Activity, Mental Engagement, and Diet Promote Cognitive Health during Aging. Neural Plast. 2017;2017.
201. Rendeiro C, Rhodes JS, Spencer JP. The mechanisms of action of flavonoids in the brain: Direct versus indirect effects. Neurochem Int. 2015;89:126-39.
202. Kim SJ, Son TG, Park HR, Park M, Kim MS, Kim HS, et al. Curcumin stimulates proliferation of embryonic neural progenitor cells and neurogenesis in the adult hippocampus. J Biol Chem. 2008;283:14497-505.
203. Sharma S, Ying Z, Gomez-Pinilla F. A pyrazole curcumin derivative restores membrane homeostasis disrupted after brain trauma. Exp Neurol. 2010;226:191-9.
204. Pu Y, Zhang H, Wang P, Zhao Y, Li Q, Wei X, et al. Dietary curcumin ameliorates aging-related cerebrovascular dysfunction through the AMPK/uncoupling protein 2 pathway. Cell Physiol Biochem. 2013;32:1167-77.
205. Cheng YF, Guo L, Xie YS, Liu YS, Zhang J, Wu QW, et al. Curcumin rescues aging-related loss of hippocampal synapse input specificity of long term potentiation in mice. Neurochem Res. 2013;38:98-107.
206. Cox KH, Pipingas A, Scholey AB. Investigation of the effects of solid lipid curcumin on cognition and mood in a healthy older population. J Psychopharmacol. 2015;29:642-51.
207. Jelenkovic A, Jovanovic MD, Stevanovic I, Petronijevic N, Bokonjic D, Zivkovic J, et al. Influence of the green tea leaf extract on neurotoxicity of aluminium chloride in rats. Phytother Res. 2014;28:82-7.
208. Gundimeda U, McNeill TH, Fan TK, Deng R, Rayudu D, Chen Z, et al. Green tea catechins potentiate the neuritogenic action of brain-derived neurotrophic factor: role of 67-kDa laminin receptor and hydrogen peroxide. Biochem Biophys Res Commun. 2014;445:218-24.
209. Xie W, Ramakrishna N, Wieraszko A, Hwang YW. Promotion of neuronal plasticity by (-)-epigallocatechin-3-gallate. Neurochem Res. 2008;33:776-83.
210. Haque AM, Hashimoto M, Katakura M, Tanabe Y, Hara Y, Shido O. Long-term administration of green tea catechins improves spatial cognition learning ability in rats. J Nutr. 2006;136:1043-7.
211. Kesse-Guyot E, Fezeu L, Andreeva VA, Touvier M, Scalbert A, Hercberg S, et al. Total and specific polyphenol intakes in midlife are associated with cognitive function measured 13 years later. J Nutr. 2012;142:76-83.
212. Wang Z, Gu J, Wang X, Xie K, Luan Q, Wan N, et al. Antidepressant-like activity of resveratrol treatment in the forced swim test and tail suspension test in mice: the HPA axis, BDNF expression and phosphorylation of ERK. Pharmacol Biochem Behav. 2013;112:104-10.
213. Liu D, Xie K, Yang X, Gu J, Ge L, Wang X, et al. Resveratrol reverses the effects of chronic unpredictable mild stress on behavior, serum corticosterone levels and BDNF expression in rats. Behav Brain Res. 2014;264:9-16.
214. Yazir Y, Utkan T, Gacar N, Aricioglu F. Resveratrol exerts anti-inflammatory and neuroprotective effects to prevent memory deficits in rats exposed to chronic unpredictable mild stress. Physiol Behav. 2015;138:297-304.
215. Witte AV, Kerti L, Margulies DS, Floel A. Effects of resveratrol on memory performance, hippocampal functional connectivity, and glucose metabolism in healthy older adults. J Neurosci. 2014;34:7862-70.
216. Eccles JC. Interpretation of action potentials evoked in the cerebral cortex. Electroencephalogr Clin Neurophysiol. 1951;3:449-64.
Latest peer-reviewed papers
AU: Henry Pollard, BSc, Grad Dip Chiro, Grad Dip App Sc, M Sport Sc, PhD, ICSSD, FICC, FAICE. Adjunct Professor, Durban University of Technology. e: drhenrypollard@gmail.com
Narrative:Joint hypermobility is common and frequently under-recognised in Chiropractic practice. This review defines joint laxity and hypermobility, presents mobility as a clinical spectrum, outlines major conditions associated with symptomatic hypermobility, and summarises evidence-based assessment and management strategies relevant to chiropractors.
Hypermobility exists on a continuum from asymptomatic increased range to disabling instability. Reliable tools include the Beighton score, validated screening questionnaires, and limb-specific assessments. Hypermobility predisposes to recurrent dislocations, patellar instability, chronic ankle sprains, and secondary overload syndromes such as rotator cuff tendinopathy.
Spinal laxity also occurs in connective tissue disorders and degenerative lumbar instability. Evidence supports rehabilitation focused on strengthening, proprioception, pacing, and education.
Spinal manipulation may provide short-term analgesia but repeated thrust techniques in unstable joints may worsen symptoms and disability trajectories over time. Chiropractors play an important role in recognising hypermobility, avoiding inappropriate mobilisation of unstable segments, and delivering evidence-based care centred on functional stability.
Indexing terms: Chiropractic; joint hypermobility; hypermobility spectrum disorder; Ehlers-Danlos syndrome; manipulation; adjustment, rehabilitation; instability.
Cite: Pollard H. Joint Hypermobility in Chiropractic Practice: Spectrum, Recognition, Spinal and Extremity Laxity, and Evidence-Based Care. Asia-Pac Chiropr J. 2026;7.1. https://www.apcj.site/PollardJointHypermobility.pdf
Introduction
Joint hypermobility is common in the general population. For many people, it causes no problems at all. They are simply flexible. Others, however, experience pain, instability, repeated injury, and long-term disability. In these patients, hypermobility becomes clinically important. This is especially relevant in chiropractic practice, where patients often present with persistent musculoskeletal pain that does not fit simple mechanical patterns. (1)
Hypermobility is not a diagnosis by itself. It is a physical trait. Its meaning depends on context. Some individuals have increased joint motion without symptoms, while others develop complex syndromes involving connective tissue, proprioceptive impairment, fatigue, and multisystem complaints. (2) These symptomatic forms are now grouped under modern classifications of hypermobility-related disorders. (1)
For Chiropractors, recognising hypermobility is essential. It influences clinical reasoning, risk assessment, and treatment planning. Spinal and extremity manipulation may provide short-term pain relief, but in unstable joints, repeated mobilisation may worsen irritability and functional outcomes over time. (3) Understanding when mobility is adaptive, and when it signals instability, is therefore a core clinical skill.
This review provides a practical and evidence-based framework for Chiropractors. It defines laxity and hypermobility, explains the spectrum of joint mobility, outlines conditions associated with symptomatic hypermobility, and discusses assessment and management options supported by peer-reviewed research.
Definitions
Joint Laxity and Joint Hypermobility
Joint laxity refers to excessive passive movement within a joint due to reduced stiffness of supporting structures such as ligaments, capsules, or connective tissue restraints. It is primarily a structural concept. Laxity is important because it reduces passive stability, meaning that joints rely more heavily on muscular control to remain aligned during movement. (4)
Laxity is clinically relevant in extremity and spinal disorders. In the shoulder, laxity contributes to multidirectional instability and recurrent subluxation. (5) In the knee, laxity can predispose to patellar instability. (6) In the lumbar spine, segmental laxity plays a role in degenerative instability trajectories. (7) Joint laxity is therefore not simply ‘extra movement’, it is a biomechanical vulnerability.
Joint hypermobility describes the ability of a joint to move beyond expected physiological limits, accounting for age, sex, and ethnicity. (2) It is a clinical finding rather than a disease. Hypermobility may be localised to one region or generalised across multiple joints.
Some hypermobility is benign. However, when hypermobility is accompanied by pain, instability, fatigue, or functional impairment, it becomes part of a broader clinical syndrome. Modern classification recognises this spectrum through hypermobility spectrum disorders and hypermobile Ehlers-Danlos syndrome. (1) The distinction matters. A flexible dancer with no symptoms is not the same as a patient with recurrent dislocations and chronic pain.
Hypermobility spectrum disorders and hypermobile Ehlers-Danlos syndrome
The 2017 classification of the Ehlers-Danlos syndromes clarified diagnostic criteria for hypermobile EDS and positioned hypermobility spectrum disorders as symptomatic hypermobility that does not meet hEDS criteria. (1, 8) Hypermobility spectrum disorders are common in musculoskeletal practice and often present with pain, instability, proprioceptive impairment, and reduced functional tolerance. (2)
Subluxation
Medical and Chiropractic concepts
The term subluxation has different meanings in different clinical contexts. In medicine and orthopaedics, subluxation refers to a partial dislocation where joint surfaces lose normal anatomical alignment. This is a structural diagnosis, commonly associated with trauma or connective tissue disorders, and is often confirmed radiologically. (9)
In Chiropractic, the WHO guideline definition describes subluxation as:
a lesion or dysfunction in a joint or motion segment in which alignment, movement integrity and/or physiological function are altered while contact between joint surfaces remains intact. It is described as a functional entity that may influence biomechanical and neural integrity, and the purported displacement is not necessarily visible on static imaging. (10)
This distinction is critical in hypermobility care. In unstable hypermobile joints, the clinical problem is not a fixed displacement to correct. The problem is insufficient restraint and poor control. Management must prioritise stability rather than repeatedly increasing motion.
Clinical relevance for Chiropractors
Hypermobility challenges traditional assumptions in manual therapy. More motion is not always better. In symptomatic patients, the goal is often control, not mobility.
Spinal manipulation may reduce pain through neurophysiological mechanisms, including modulation of pain sensitivity. (11) However, manipulation does not restore ligament stiffness or passive restraint. (3) In hypermobile and unstable joints, repeated end-range mobilisation may contribute to worsening irritability and functional decline over time. (3) Recognising hypermobility early allows chiropractors to avoid inappropriate thrust techniques, prioritise stabilisation, and refer appropriately when systemic risk is suspected.
Mobility as a clinical spectrum and conditions associated with hypermobility
Joint mobility is not best understood as normal versus abnormal. In reality, movement exists along a continuum. Some joints move more than expected, some less, and both extremes can generate clinical problems.
At one end of this spectrum lies unstable hypermobility. Here, joint motion exceeds normal limits and is accompanied by reduced connective tissue restraint and impaired neuromuscular control. Patients often describe joints that feel unreliable. Sprains recur easily. Episodes of giving way or dislocation may occur without major trauma. (2)
In the middle lies stable mobility. This is the zone of healthy function. Joints move freely but remain well supported by passive structures and coordinated muscle control. Load tolerance is high. Symptoms are minimal.
At the opposite end lies hypomobility. Restricted motion is often linked with stiffness, protective guarding, or degenerative adaptation. In the spine, this may contribute to segmental overload and adjacent compensation over time. (7)
These states often coexist. Hypermobile patients frequently develop stiff protective regions, especially in the spine. (3) Excess motion in one segment may coexist with restriction in another. This complexity explains why simplistic approaches, such as treating every painful area as a site of restriction, can fail in hypermobile care.
Figure 1: Joint mobility as a clinical spectrum (unstable hypermobility to stable mobility to hypomobility).
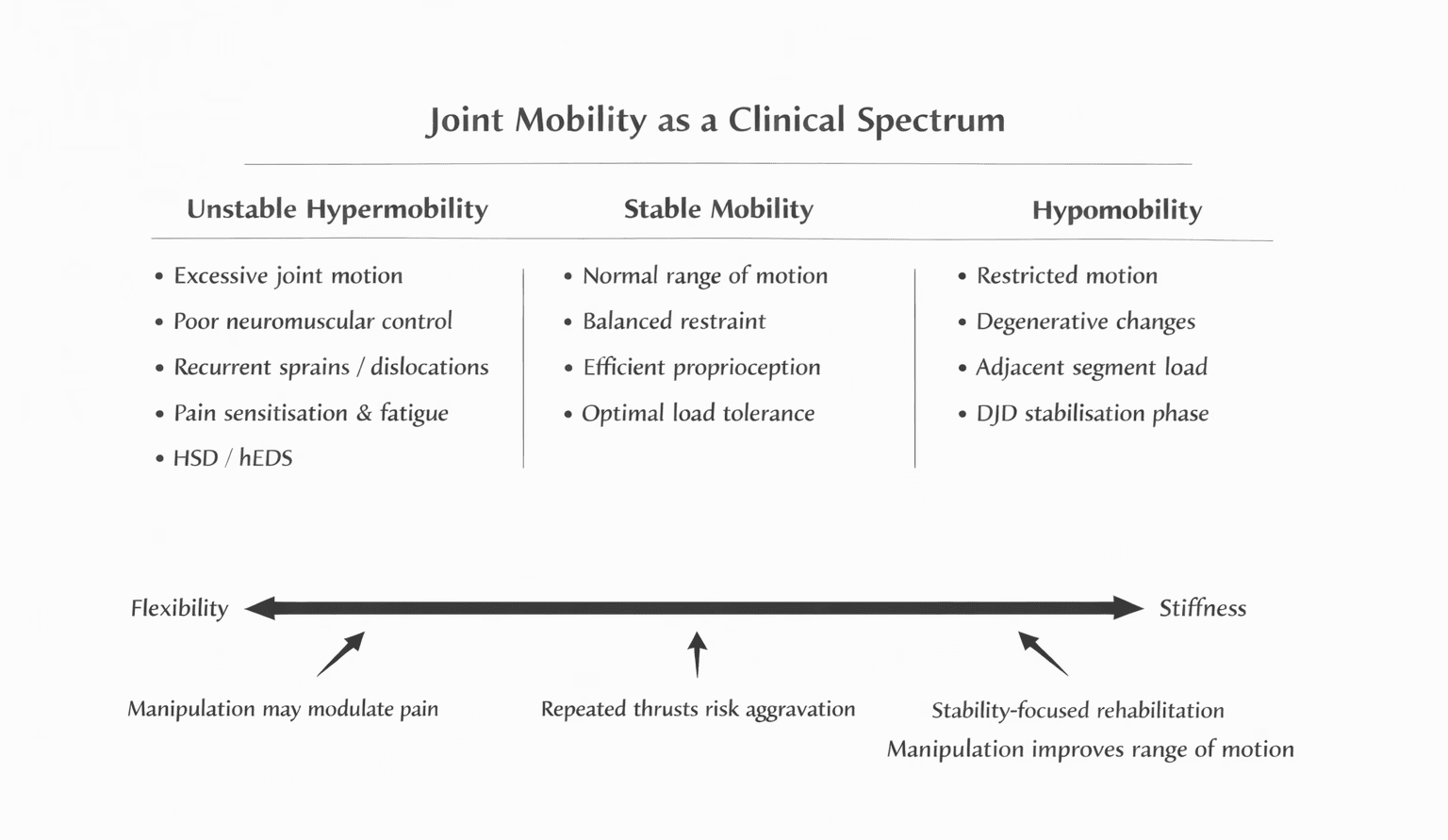
Not all hypermobility is inherited. Joint laxity can also be acquired after injury or physiologic change, including pregnancy-related ligamentous change. (17) Repetitive end-range stretching may worsen restraint in predisposed individuals. This is clinically relevant because flexibility-focused programmes can unintentionally increase instability.
Table 1: Clinical factors relevant to hypermobility recognition (Part 1)
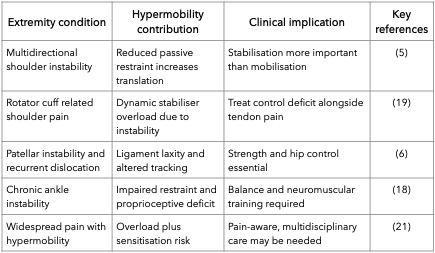
Extremity manifestations are among the most disabling aspects of symptomatic hypermobility. Pain is often not caused by restriction. It is caused by excess motion without control.
Spinal Laxity, Degenerative Instability, and Disability Trajectories
Hypermobility is often discussed in relation to the extremities. However, spinal laxity is equally important. Chiropractors frequently manage spinal pain, and hypermobility in spinal segments changes both diagnosis and treatment risk.
Spinal stability reflects a balance between passive restraints, muscular control, and neural coordination. (22) Painful segments in hypermobile patients may represent the point of load failure within a broader kinetic chain rather than the sole source of dysfunction. (23) When passive support is compromised, the system relies more heavily on active control. In practice, painful segments in hypermobile patients may represent the point of load failure within a broader kinetic chain rather than the sole source of dysfunction.
Spinal hypermobility in heritable disorders
In hypermobile EDS and related disorders, spinal pain is common and may be accompanied by fatigue and broader pain burden. (8, 24) Proprioceptive impairment also affects spinal control and may contribute to recurrent pain episodes. (20)
Upper cervical involvement requires special caution. Neurological and spinal manifestations of EDS have been described, and suspected craniocervical instability requires referral rather than thrust manipulation. (25)
Degenerative joint disease and instability
A common misconception is that degeneration always produces stiffness. Degenerative spinal change often passes through an instability phase in which excessive motion contributes to pain recurrence and disability. (7) This is clinically relevant in older adults and in disabled populations where instability and deconditioning interact.
Motor control impairment is strongly linked with chronic spinal pain. Hodges and Richardson demonstrated inefficient deep trunk stabilisation associated with low back pain. (26) Exercise therapy has strong evidence for non-specific chronic low back pain and aligns with stabilisation-oriented care. (27)
In both heritable and degenerative contexts, excess motion may be the problem, not restriction.
Clinical recognition and assessment of hypermobility
Hypermobility is frequently missed in routine musculoskeletal care. Many patients are treated for isolated pain sites without recognition of the underlying stability problem.
Recognition begins with history. Patients often describe lifelong patterns rather than acute onset problems. They may recall being ‘double-jointed’ as children, with symptoms increasing over time. (2)
History features suggestive of symptomatic hypermobility include recurrent sprains, repeated instability episodes, or dislocations with minimal trauma. (5) Pain may be diffuse, shifting, and accompanied by tendon complaints that do not resolve with standard care. (19) Fatigue and autonomic symptoms may be prominent in hEDS. (13) Psychological distress may also occur, including anxiety vulnerability. (15)
Examination
The Beighton score is widely used to assess generalised joint hypermobility. (28) However, Beighton alone has limitations. It does not capture limb-specific instability, proprioception, or functional control deficits. Clinical assessment should include movement quality, mid-range control, and stabiliser endurance.
The 5-part questionnaire is a useful screening adjunct, particularly in adults who may have stiffened with age. (29) Limb-specific tools such as the Lower Limb Assessment Score improve detection of lower extremity hypermobility. (30) Proprioceptive deficits are well documented and support including joint position sense and balance testing in assessment. (20)
Referral awareness is essential when systemic risk is suspected, including severe autonomic symptoms or suspected cervical instability. (13, 25)
Table 2: Clinical tools for recognition and assessment
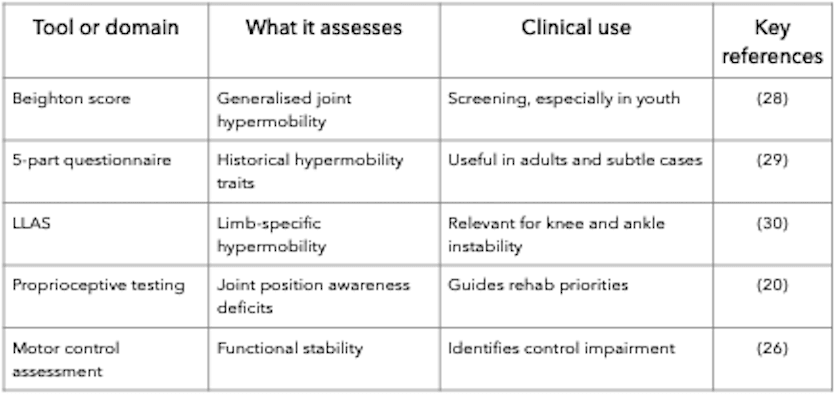
Manipulation
Short-term benefit, contraindications, and long-term risk
Detailed discussion of manipulation safety and rehabilitation strategies is presented in Part 2 of this review. Spinal adjustment / manipulation is central to Chiropractic practice. In people with hypermobility, it raises a clinical question. When does mobilisation relieve pain safely, and when might it aggravate an unstable system?
Manual therapy can provide short-term symptom improvement through neurophysiological mechanisms. Manipulation influences pain processing and may reduce guarding and pain sensitivity. (11) These responses explain immediate relief in some hypermobile patients.
The difficulty is that pain relief does not necessarily indicate improved stability.
Manipulation / adjustment does not restore ligament stiffness or passive restraint. (3) This does not mean manipulation has no role in care, but rather that its effects should be interpreted primarily as short-term symptom modulation rather than structural correction. In symptomatic hypermobility, excess motion without adequate neuromuscular control is often the primary impairment. (3)
Caution is required where restraint is severely compromised. Suspected craniocervical instability is a major contraindication to high-velocity cervical manipulation/adjustment and requires referral. (25) Degenerative lumbar instability is also relevant. Degeneration can include an instability phase during which excessive motion contributes to pain recurrence and disability.(7) In such contexts, repeated mobilisation at unstable levels may increase irritability rather than improve function.
Autonomic dysfunction also complicates care. Orthostatic intolerance and syncope warrant careful screening and conservative approaches. (13) Recurrent dislocation syndromes indicate that passive restraint has already failed, and further mobilisation is unlikely to address the core impairment. (5)
This does not remove the Chiropractor’s role, it refines it. Manual therapy may still be useful when applied selectively to coexisting hypomobile regions or for symptom modulation when applying a ‘kinetic chain’ approach to care (covered in part 2). The long-term focus should shift toward stabilisation and active rehabilitation.
Figure 2: Situations where manipulation should not be used in hypermobility.
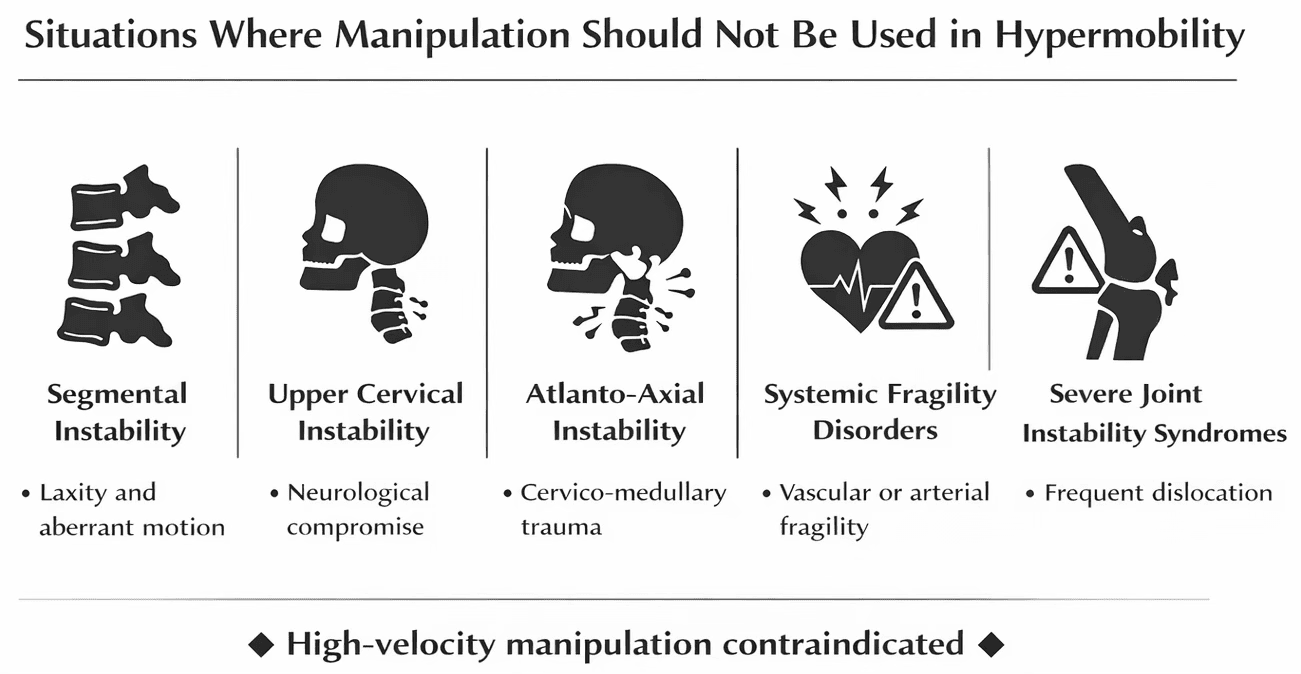
Evidence-Based Rehabilitation and Management
The most effective interventions in symptomatic hypermobility improve control, strength, and functional tolerance. Hypermobility is not primarily a mobility problem. It is a stability problem.
Strength and resistance training
Progressive strengthening improves active stability and reduces symptoms. Trials in children with hypermobility have shown benefits from strengthening and proprioceptive programmes, including reduced knee pain and improved function. (31)
Proprioceptive and sensorimotor rehabilitation
Proprioceptive deficits are common and clinically meaningful. (20) Enhancement of proprioception has been shown to improve symptoms in hypermobility syndromes. (4) Balance training, perturbation work, and closed-chain control are central.
Motor control and spinal stabilisation
Deep stabiliser impairment is associated with chronic low back pain. (26) Exercise therapy has strong evidence in non-specific low back pain and aligns with stabilisation-oriented care for instability-driven presentations. (27) These principles map onto spinal stability models emphasising passive, active, and neural subsystems. (22)
Multidisciplinary care and pacing
Multidisciplinary approaches combining physical and cognitive-behavioural strategies have improved disability outcomes in hypermobility-related conditions. (32) Psychological therapies have evidence in chronic and recurrent pain, supporting pacing and function-oriented recovery. (33) Pain management frameworks in EDS emphasise coordinated strategies over passive-only care. (21)
What is not supported
Passive-only care does not address the underlying impairment. Stretching programmes aimed at increasing flexibility may be inappropriate in already hypermobile patients. Repeated thrust manipulation/adjustment into lax segments may provide short-term analgesia but does not restore restraint and may worsen irritability over time. (3)
Chiropractic care is most effective when it includes education, graded strengthening, proprioception, pacing, and load management.
Conclusion and Practice Recommendations
Joint hypermobility is common, but its clinical meaning varies widely. For some individuals it is benign. For others, it drives persistent pain, instability, recurrent injury, and disability. Recognising this difference is essential in Chiropractic practice.
Hypermobility is best conceptualised as a spectrum from unstable hypermobility to stable mobility to hypomobility. Extremity laxity increases risk of recurrent dislocation and secondary overload syndromes such as tendinopathy, including rotator cuff related pain and patellar instability. Spinal laxity may occur in heritable connective tissue disorders and during degenerative instability trajectories.
Validated screening tools and careful history and examination improve detection. Autonomic dysfunction and suspected cervical instability require conservative decision-making and appropriate referral.
Manipulation may provide short-term analgesia via neurophysiological mechanisms. (11) However, manipulation does not restore ligament stiffness or passive restraint. (3) In unstable joints, repeated end-range mobilisation may worsen irritability and functional outcomes over time. (3) Evidence supports stabilisation-oriented rehabilitation, including progressive strengthening, proprioceptive retraining, pacing, and patient education.
Hypermobility is not primarily a mobility problem. It is a stability problem. Chiropractors who recognise this early can improve safety and outcomes by prioritising control, confidence, and long-term function.
References
- Malfait F, Francomano CA, Byers PH, et al. The 2017 international classification of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):8-26.
- Castori M, Tinkle B, Levy H, et al. A framework for the classification of joint hypermobility and related conditions. Am J Med Genet C Semin Med Genet. 2017;175(1):148-157.
- Simmonds JV, Keer RJ. Hypermobility and the hypermobility syndrome. Man Ther. 2007;12(4):298-309.
- Ferrell WR, Tennant N, Sturrock RD, et al. Amelioration of symptoms by enhancement of proprioception in patients with joint hypermobility syndrome. Arthritis Rheum. 2004;50(10):3323-3328.
- Cameron KL, Duffey ML, DeBerardino TM, et al. Association of generalized joint hypermobility with a history of glenohumeral joint instability. J Athl Train. 2010;45(3):253-258.
- Lafave MR, Hiemstra LA, Kerslake S. Association between generalized joint hypermobility and patellar instability outcomes. Knee Surg Sports Traumatol Arthrosc. 2019;27(9):2935-2942.
- Kirkaldy-Willis WH, Farfan HF. Instability of the lumbar spine. Clin Orthop Relat Res. 1982;(165):110-123.
- Tinkle B, Castori M, Berglund B, et al. Hypermobile Ehlers-Danlos syndrome (a.k.a. Ehlers-Danlos syndrome type III and Ehlers-Danlos syndrome hypermobility type): clinical description and natural history. Am J Med Genet C Semin Med Genet. 2017;175(1):48-69.
- Beighton P, Horan F. Orthopaedic aspects of the Ehlers-Danlos syndrome. J Bone Joint Surg Br. 1969;51(3):444-453.
- World Health Organization. WHO guidelines on basic training and safety in chiropractic. Geneva: WHO; 2005. Date accessed: cited 2026 Mar 4. Available from: https://iris.who.int/handle/10665/43352
- Pickar JG. Neurophysiological effects of spinal manipulation. Spine J. 2002;2(5):357-371.
- Remvig L, Jensen DV, Ward RC. Epidemiology of general joint hypermobility and basis for proposed criteria for benign joint hypermobility syndrome: review. J Rheumatol. 2007;34(4):804-809.
- De Wandele I, Rombaut L, Malfait F, et al. Orthostatic intolerance and fatigue in the hypermobility type of Ehlers-Danlos syndrome. Rheumatology (Oxford). 2016;55(8):1412-1420.
- Mathias CJ, Low DA, Iodice V, et al. Postural tachycardia syndrome: current experience and concepts. J Neurol Neurosurg Psychiatry. 2012;83(8):872-880.
- Bulbena A, Gago J, Pailhez G, et al. Joint hypermobility as a risk trait for anxiety disorders: a review. Gen Hosp Psychiatry. 2011;33(4):363-370.
- Bulbena A, Duró JC, Porta M, et al. Anxiety disorders in the joint hypermobility syndrome. Psychiatry Res. 1993;46(1):59-68.
- Schauberger CW, Rooney BL, Goldsmith L, et al. Peripheral joint laxity increases in pregnancy but does not correlate with pelvic floor outcomes. Obstet Gynecol. 1996;88(4 Pt 1):635-639.
- Hertel J. Functional instability following lateral ankle sprain. J Athl Train. 2002;37(4):364-375.
- Lewis JS. Rotator cuff related shoulder pain: assessment, management and uncertainties. Man Ther. 2016;23:57-68.
- Rombaut L, De Paepe A, Malfait F, et al. Joint position sense and vibratory perception in patients with Ehlers-Danlos syndrome hypermobility type. Clin Rheumatol. 2010;29(3):289-295.
- Chopra P, Tinkle B, Hamonet C, et al. Pain management in the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):212-219.
- Panjabi MM. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement. J Spinal Disord. 1992;5(4):383-389.
- Kibler WB, Press J, Sciascia A. The role of core stability in athletic function. Sports Med. 2006;36(3):189-198.
- Scheper MC, de Vries JE, Verbunt J, et al. Chronic pain in hypermobility syndrome and Ehlers-Danlos syndrome (hypermobility type): it is a challenge. J Pain Res. 2015;8:591-601.
- Henderson FC Sr, Austin C, Benzel E, et al. Neurological and spinal manifestations of the Ehlers-Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017;175(1):195-211.
- Hodges PW, Richardson CA. Inefficient muscular stabilization of the lumbar spine associated with low back pain: a motor control evaluation of transversus abdominis. Spine (Phila Pa 1976). 1996;21(22):2640-2650.
- Hayden JA, van Tulder MW, Malmivaara A, et al. Exercise therapy for treatment of non-specific low back pain. Ann Intern Med. 2005;142(9):765-775.
- Beighton P, Solomon L, Soskolne CL. Articular mobility in an African population. Ann Rheum Dis. 1973;32(5):413-418.
- Hakim AJ, Grahame R. A simple questionnaire to detect hypermobility: an adjunct to the assessment of patients with diffuse musculoskeletal pain. Int J Clin Pract. 2003;57(3):163-166.
- Ferrari J, Parslow C, Lim E, Hayward A. Joint hypermobility: the use of a new assessment tool to measure lower limb hypermobility. Clin Exp Rheumatol. 2005 May-Jun;23(3):413-20.
- Pacey V, Tofts L, Adams RD, et al. Exercise in children with joint hypermobility syndrome and knee pain: a randomised controlled trial. Pediatr Rheumatol Online J. 2013;11:30.
- Bathen T, Hångmann AB, Hoff M, et al. Multidisciplinary treatment of disability in Ehlers-Danlos syndrome hypermobility type: a pilot study. Am J Med Genet A. 2013;161A(12):3005-3011.
- Eccleston C, Fisher E, Craig L, et al. Psychological therapies for the management of chronic and recurrent pain in children and adolescents. Cochrane Database Syst Rev. 2014;(5):CD003968.
AU 1: Gilbert Weiner, DC, LST, FFCLB. Adjunct Assistant Professor, Northeast College of Health Sciences. Private Practice, Bellingham, MA. e: drweiner@hotmail.com
AU 2: Charles L Blum, DC. Director of Research, Sacro Occipital Technique Organization - USA. Private practice of Chiropractic, Santa Monica, CA.
Purpose: To investigate the relationship between C2 slope and pelvic tilt and provide clinicians with an additional radiographic parameter for evaluating global spinal balance using routine lateral cervical imaging.
Methods: Incorporating cervical analysis into full-spine evaluations may improve diagnostic accuracy when addressing persistent pelvic imbalance or recurrent postural compensations. For practitioners utilising Sacro Occipital Technique, these findings offer a measurable framework that may support traditional clinical observations regarding the cranial-pelvic relationship.
Conclusions: Assessment of C2 alignment may help identify compensatory postural adaptations that influence pelvic orientation and overall sagittal integrity Further clinical investigation may clarify whether evaluating C2 alignment prior to pelvic category correction could enhance stability and longevity of chiropractic adjustments.
Indexing terms: Chiropractic spinal adjustment; Sacro-Occipital Technique (SOT), C2 slope, Myodural bridge, cerebral spinal fluid flow, Dural torque.
Cite: Weiner G, Blum CL. Is the C2 slope a reliable indicator of decompensated spinopelvic alignment? A Sacro Occipital Technique perspective. Asia-Pac Chiropr J. 2026;7.1 https://www.apcj.site/WeinerC2slope.pdf
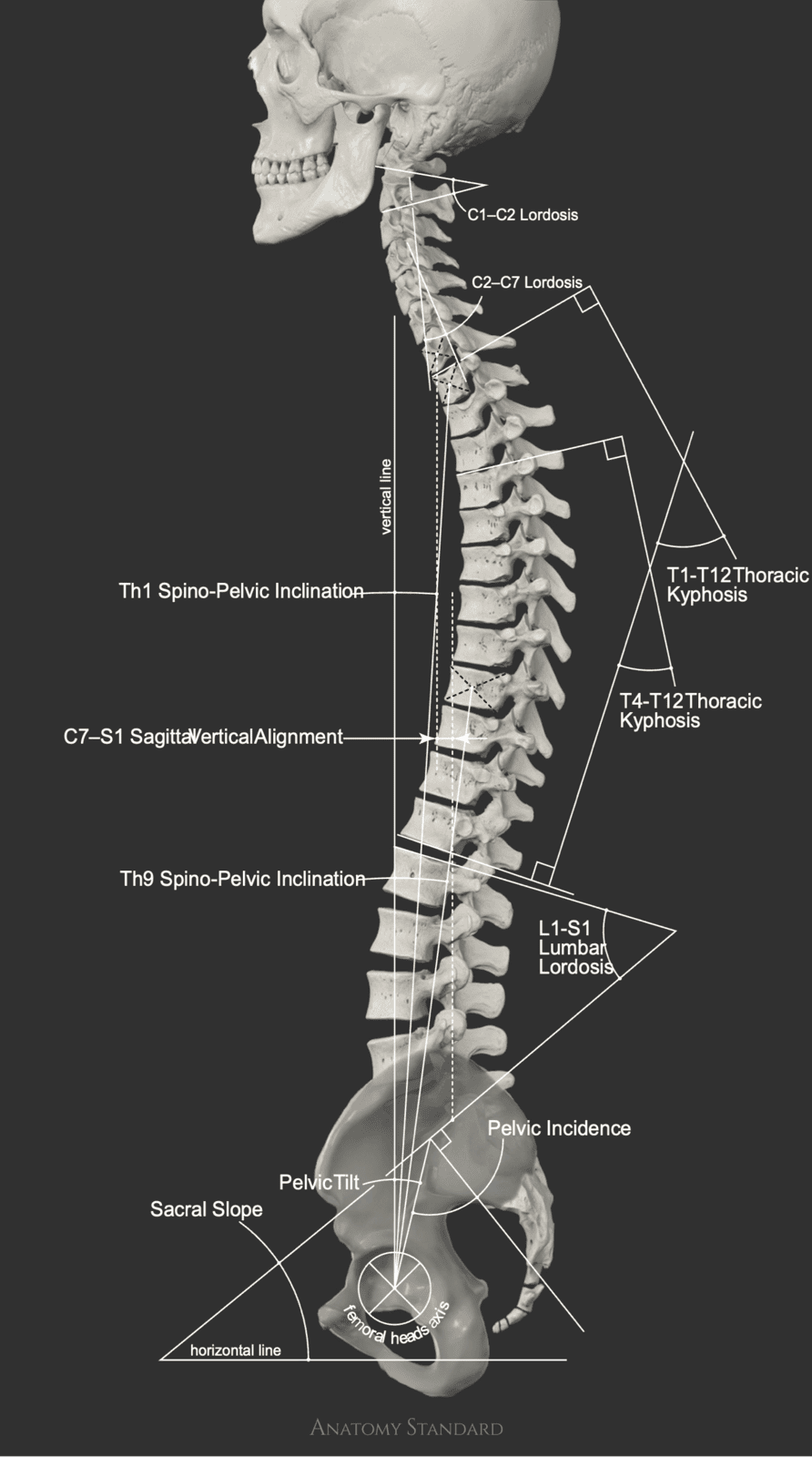
Clinical implications
Introduction
A growing body of research has illustrated an intimate connection between the C2 slope and pelvic tilt (PT). (1, 2, 3, 4) One study reports unequivocally that ‘C2 slope (C2S) is a critical, easily measured radiographic marker that can be used in cervical sagittal alignment analysis and serves as a simplified, accurate calculation for pelvic tilt (PT)’. (5) As shown in Figure 1 above, it acts as a vital link between the upper and lower spine and pelvic position, assisting clinicians in the diagnosis of spinal deformity. Furthermore, it has been reported that when the C2 pelvic angle (C2PA) exceeds 13°–16°, it becomes a reliable indicator of decompensated spinopelvic alignment, often correlating with poorer patient-reported outcomes, including lower SF-36 scores and increased pain. (6, 7)
These findings provide clinicians with a rapid and reliable method for assessing spinal sagittal integrity, often within one degree of accuracy, using only a lateral cervical radiograph. One radiographic study of volunteers with both high and low pelvic incidence demonstrated that, despite extreme variations in pelvic parameters, C2 tilt remained within 1° of L1 pelvic angles. (5)
Reconsidering the earlier observations of DeJarnette within Sacro Occipital Technique (SOT), the pelvis and the head were proposed to be intimately connected. (8) What is remarkable is that these concepts were developed purely through radiographic interpretation and clinical observation, without the benefit of modern imaging software, computational modelling, or advanced statistical analysis. DeJarnette demonstrated a keen understanding of body mechanics and compensatory mechanisms, recognising that a functional relationship must exist between cranial and pelvic structures.
When C2 tilts forward, represented radiographically by an increased C2 slope, the body may compensate by tilting the pelvis posteriorly in order to maintain balance and preserve visual and vestibular cerebellar postural reflexes. This compensation assists the body in maintaining equilibrium in response to gravity. (9)
Several neurological reflexes help explain this C2–pelvic relationship.
The Asymmetrical Tonic Neck Reflex (ATNR)
The Asymmetrical Tonic Neck Reflex (ATNR) contributes to pelvic symmetry during development by linking head rotation (guided primarily by C1–C2 motion) to contralateral limb extension and pelvic shifts. (10)
The Symmetrical Tonic Neck Reflex (STNR)
The Symmetrical Tonic Neck Reflex (STNR) regulates muscular tone in response to cervical flexion and extension. Neck flexion promotes arm flexion and leg extension, influencing sagittal pelvic positioning. (10)
The Cervicocollic Reflex (CCR) and vestibulospinal reflexes
The Cervicocollic Reflex (CCR) and vestibulospinal reflexes stabilise head position, and their neural input modulates lumbar and pelvic musculature. Within this framework, C2 misalignment may disrupt these reflex pathways, potentially leading to compensatory pelvic tilts that help maintain overall postural balance. (11)
The Spinal Galant Reflex
The Spinal Galant Reflex, primarily active in infancy to facilitate pelvic mobility, may also influence hip and pelvic tilt if retained beyond early development. (12)
The cervicolumbar reflex
Additionally, the cervicolumbar reflex involves neural pathways linking proprioceptive input from cervical muscles and ligaments, particularly those near C2, to the lower spine and pelvis. These pathways provide feedforward control, enabling the brain to anticipate changes in pelvic positioning based on cervical posture to maintain balance. (13)
Clinically, Chiropractic techniques have long recognised functional spinal relationships that contribute to postural stability. In SOT, the Lovett Brother phenomenon, described as R + C factors, suggests that vertebral segments function in paired relationships to maintain spinal balance. (14, 15) Within this clinical model, C2 is often considered functionally coupled with L4. In this relationship, C2 may exert a descending influence on L4 positioning, while L4 may exert an ascending influence on C2.
The L4 vertebra also plays an important role in pelvic tilt by influencing the lumbosacral angle. Dysfunction at the L4/L5 segment can contribute to anterior or lateral pelvic tilt, increasing mechanical stress on the lower back and potentially leading to pain. (16) Structural alterations at L4/L5 or L5/S1 may cause the sacral base to become unlevel, producing compensatory pelvic tilt.
From a neuroanatomical perspective, the C2 facet joints, the first true facet joints in the cervical spine, as C1 lacks typical facets, are critical for cervical proprioception. These joints provide essential afferent input regarding head position and play a key role in stabilising motion to protect neural structures. They are densely populated with mechanoreceptors and function in conjunction with deep cervical musculature to regulate posture and balance throughout the spinal column, extending influence to the pelvis. (9)
The upper cervical spine, particularly the C2 facet joints and surrounding musculature, contains a high concentration of mechanoreceptors such as Pacinian corpuscles and Golgi tendon organs. These receptors provide continuous sensory input to the central nervous system regarding head position, enabling coordinated spinal balance and movement. Dysfunction within these structures, resulting from injury, degeneration, or subluxation, may impair cervical repositioning sense and force compensatory adjustments within the lower spine and pelvis. (17)
In evaluating cranial-pelvic balance, it is therefore necessary to consider all anatomical and myofascial structures that influence this relationship. For this reason, SOT practitioners often palpate and evaluate the longitudinal occipital myofascial fibres along the occipital bone. (18)
Neuro-anatomically, the greater occipital nerve (GON) arises from the C2 spinal nerve and travels between the obliquus capitis inferior and semispinalis capitis muscles. Although primarily sensory, supplying the posterior scalp, it also influences suboccipital musculature. Irritation or entrapment of this nerve, commonly occurring near the C2 level, may result in occipital neuralgia, characterised by scalp pain or hypersensitivity. (19)
Additionally, the lesser occipital nerve, which originates from the cervical plexus (primarily C2), supplies sensation to the lateral occipital region extending toward the posterior auricular area. (19)
Taken together, these anatomical and neurological relationships suggest another measurable parameter that may be incorporated into a comprehensive spine-to-pelvis evaluation. Within a full-spine clinical model, such as that advocated in Sacro Occipital Technique, postural balance and autonomic nervous system regulation are viewed as interdependent components of a unified biomechanical system.
Radiographic Measurement of C2 Slope and Pelvic Tilt
The measurement of C2 slope and pelvic tilt can be performed using standard radiographic analysis.
- Draw a line along the inferior endplate of C2 (Line C in Figure 2).
- Draw a second line along McGregor’s Line, extending from the posterior hard palate to the base of the occiput (Line A in Figure 2).
- The angle formed between these two lines represents the occiput–C2 angle.
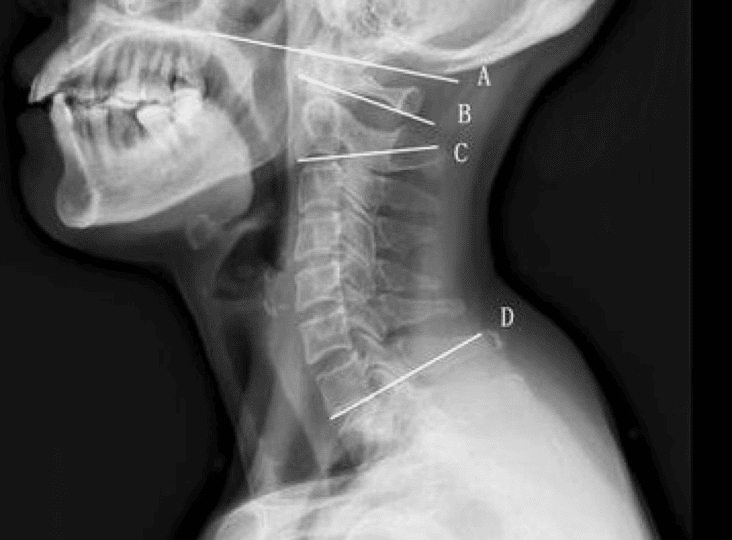
- Draw Line 1 (Vertical Axis): a vertical line passing through the midpoint between the centres of the femoral heads.
- Draw Line 2 (Pelvic Radius): a line extending from the centre of the femoral heads to the midpoint of the sacral endplate (the superior surface of the sacrum).
- The acute angle between these two lines represents the pelvic tilt (PT) (Figure 3).
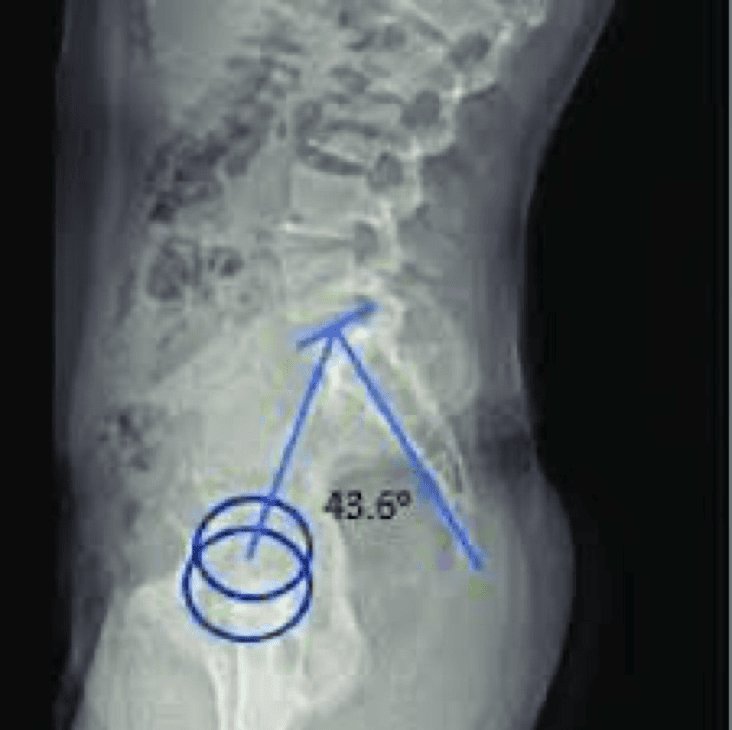
The full relationship between these measurements is illustrated in Figure 1.
The myodural bridge (MDB)
Beyond the relationship between the C2 angle and pelvic tilt, the angulation of C2 exerts additional and potentially profound effects on global spinal balance. This relationship warrants careful consideration by chiropractors in general and by practitioners of Sacro Occipital Technique (SOT) in particular. The C2 angle, specifically the O/C2 or craniocervical angle, has a significant influence on the function of the myodural bridge (MDB). Misalignment or altered angulation at C2 may generate abnormal mechanical stress on the cervical dura through the rectus capitis posterior minor and major (RCPm, RCPma) and the obliquus capitis inferior (OCI) muscles. (20, 21, 22) Increased tension transmitted through these structures has been associated with chronic cervicocephalic headache syndromes, altered cerebrospinal fluid (CSF) dynamics, and increased intracranial pressure. (23)
The primary function of the MDB is believed to be the prevention of dural infolding or inward collapse during cervical extension. By maintaining dural patency, the MDB facilitates the normal circulation of CSF. Compromise of the C2 angle may impair the ability of the MDB to retract the dura appropriately, potentially resulting in abnormal contact between the dura and adjacent neural structures, including the brainstem and spinal cord. Additionally, the MDB appears to contribute to a dynamic mechanism that assists in CSF circulation during physiological head movements such as nodding. Substantial deviation in C2 alignment may disrupt this mechanism, thereby altering intracranial pressure regulation and CSF circulation. (24)
Anatomically, the myodural bridge constitutes a direct connective interface between the dura mater and the suboccipital musculature, specifically the rectus capitis posterior major and minor (RCPma, RCPm) and the obliquus capitis inferior (OCI). These muscles originate from the posterior elements of the axis, particularly the C2 spinous process, and transmit force through fascial continuities to the cervical dura. Abnormal C2 angulation or positional deviation, sometimes described clinically as ‘wandering C2’, may result in excessive mechanical traction on the dura mater via the MDB. (24)
The MDB, linking the suboccipital muscular fascia to the dura mater, contributes to both passive and active stabilisation of the spinal cord. The structural relationships between the MDB, the dura, and the spinal column are complex and suggest potential biomechanical and neurophysiological implications not only within the cranial vault but throughout the entire spinal axis and into the pelvic region.
The dura mater demonstrates firm attachments to the posterior aspects of the C2 and C3 vertebral bodies, providing structural stability to the upper spinal cord. Additional stabilisation of the spinal meninges is provided by the ligamentum nuchae, ligamenta flava, the ligaments of Hoffman, and the ligaments of Trolard, before the dural system ultimately anchors to the coccyx through the continuation of the pia mater known as the filum terminale. (25, 26, 27, 28, 29) The filum terminale traverses the sacral hiatus and contributes to anchoring the dural sac to the periosteum of the coccyx, together with the ligament of Trolard (Figure 4). This arrangement establishes a continuous anatomical and mechanical linkage between the upper cervical spine and the complex.
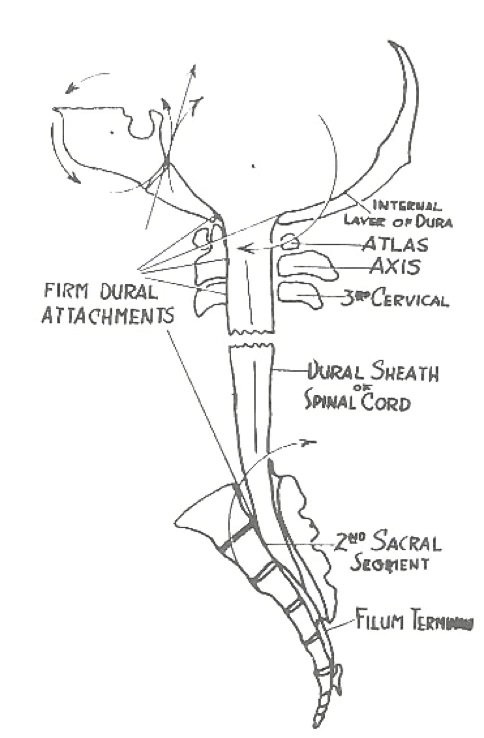
Aberrant C2 angulation may therefore influence CSF circulation and alter the mechanical integrity of the dural anchoring system, both of which represent critical focal considerations in SOT management. When C2 deviates from its normal lordotic orientation, as may occur with reduced C2–C7 lordosis or increased C2 slope and associated instability, abnormal mechanical forces may be transmitted through the MDB. Such forces may result in overstretching or functional compromise of the bridge, potentially allowing posterior displacement or compression of the dura against the brainstem. Although the C2–C7 angle is generally reported to range from approximately 13.9° to 23°, clinically meaningful changes in dural tension may occur as this relationship approaches thresholds of structural instability or in the presence of kyphotic deformity. (30)
Detailed examination of the myodural bridge–meningeal complex (Figure 5) illustrates that the posterior atlanto-occipital membrane (1) extends from the occipital bone and blends with the dura mater at the craniovertebral junction. The superior myodural bridge (2) merges with the superior vertebrodural ligament (3) of the atlas and integrates with the posterior atlanto-occipital membrane (PAOM). The PAOM represents a critical ligamentous structure at the craniovertebral junction, connecting the occiput to the atlas and contributing to cervical stability. Functionally, it acts as a continuation of the ligamentum flavum and plays an important role in limiting excessive cervical flexion. The PAOM is located at the level of the atlanto-occipital interspace. (31, 32)
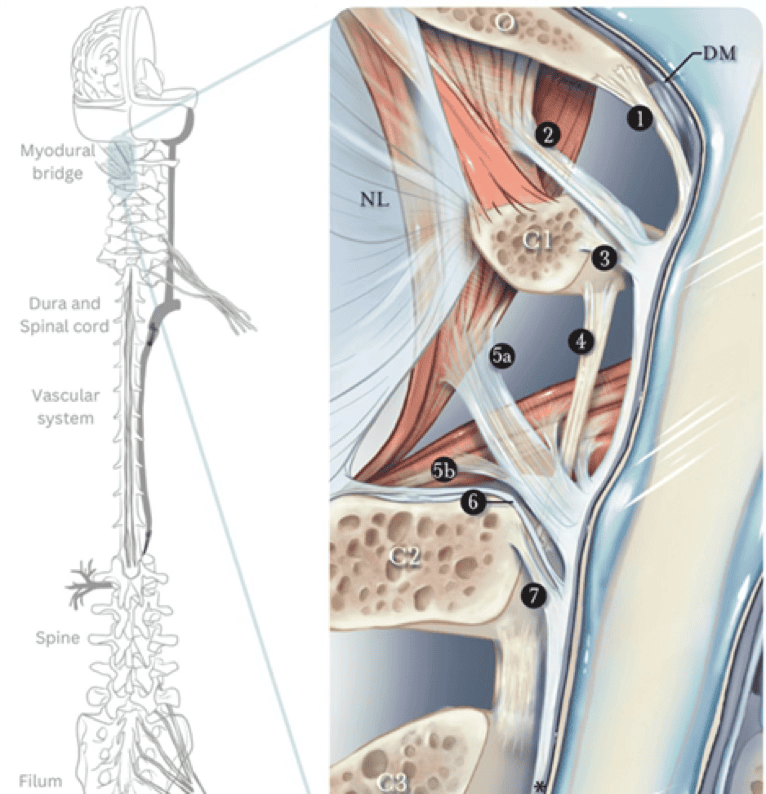
Figure 5: Neuraxial biomechanics, fluid dynamics, and myodural regulation: rethinking management of hypermobility and CNS disorders- Frost, N
Discussion
The evolution of scientific understanding often leads to the reevaluation or abandonment of earlier theoretical frameworks. Nevertheless, historical precedent demonstrates that foundational concepts developed through careful clinical observation frequently retain considerable validity. For example, ancient Greek astronomers accurately mapped planetary motion long before the invention of telescopic instrumentation, and Leonardo da Vinci conceptualised mechanical innovations centuries before technological advances made their realisation possible.
In a similar manner, early Chiropractic pioneers relied primarily on meticulous clinical observation and radiographic analysis to formulate biomechanical models of spinal function. Consequently, contemporary scientific validation should be viewed not as a replacement for earlier insights but as an opportunity to refine and contextualise them within a modern evidence-based framework.
These considerations raise several clinically relevant questions. Should clinicians routinely evaluate and, when indicated, address C2 slope or alignment prior to initiating pelvic correction? If pelvic correction is performed first, what biomechanical events occur when the patient returns to an upright posture and postural righting reflexes are immediately activated? Does the correction persist, or does the neuromusculoskeletal system rapidly reestablish preexisting compensatory patterns? Furthermore, should assessment of the C2 angle be incorporated into clinical strategies intended to influence CSF dynamics and dural tension patterns?
Conclusion
Given that Sacro Occipital Technique has been practiced for several decades with consistently favourable clinical outcomes, it is plausible that the SOT category system already accommodates the functional relationship between C2 alignment and pelvic mechanics in an integrated and adaptive manner. (33, 34) This perspective may also help explain why cervical spine adjustment is traditionally emphasised within SOT protocols following category diagnosis and treatment, and prior to the patient assuming a weight-bearing posture.
References
- Protopsaltis TS, Ramchandran S, Tishelman JC, Smith JS, Neuman BJ, Jr GMM, Lafage R, Klineberg EO, Hamilton DK, LaFage V, Gupta MC, Hart RA, Schwab FJ, Burton DC, Bess S, Shaffrey CI, Ames CP; International Spine Study Group. The Importance of C2 Slope, a Singular Marker of Cervical Deformity, Correlates With Patient-reported Outcomes. Spine (Phila Pa 1976). 2020 Feb 1;45(3):184-192.
- Hey HWD, Tan KA, Chin BZ, Liu G, Wong HK. Comparison of whole body sagittal alignment during directed vs natural, relaxed standing postures in young, healthy adults. Spine J. 2019 Nov;19(11):1832-1839.
- Kim SW, Kim TH, Bok DH, Jang C, Yang MH, Lee S, Yoo JH, Kwak YH, Oh JK. Analysis of cervical spine alignment in currently asymptomatic individuals: prevalence of kyphotic posture and its relationship with other spinopelvic parameters. Spine J. 2018 May;18(5):797-810.
- Lee SH, Son ES, Seo EM, Suk KS, Kim KT. Factors determining cervical spine sagittal balance in asymptomatic adults: correlation with spinopelvic balance and thoracic inlet alignment. Spine J. 2015 Apr 1;15(4):705-12.
- Ha A, Mathew J, Zuckerman SL, et al. 190. C2 pelvic angle (C2PA) is a useful radiographic parameter that correlates with clinical outcomes of symptomatic proximal junctional kyphosis. The Spine Journal. 2021;21(9) Supplement: Volume 21, Issue 9, Supplement:S96-S97.
- Joseph K, Bui T, Yahanda AT, Yakdan S, Vogl S, Ruiz Cardozo M, Galla JT, Leatherman Z, Poulin ND, Chakladar S, Brehm S, Benedict B, Gupta M, Pallotta N, Hills J, Kelly MP, Greenberg JK, Neuman BJ, Ray WZ, Molina CA. Validation and clinical application of the ΔC2 pelvic angle - ΔC2 tilt = Δpelvic tilt equation for predicting pelvic tilt in spinal deformity surgery. Neurosurg Focus. 2025 Jun 1;58(6):E6.
- Ouchida J, Nakashima H, Ito S, Segi N, Yamauchi I, Ode Y, Imagama S. C2 Pelvic Angle as a Predictive Measure for Decompensated Spinopelvic Alignment and Its Impact on Health-Related Quality of Life. Spine (Phila Pa 1976). 2026 Feb 15;51(4):271-279.]
- Getzoff H. A critical approach for learning the Operating Principles of Sacro Occipital Technique (SOT) Chiropractic. Asia-Pac Chiropr J. 2023;3.4.
- Morningstar MW, Pettibon BR, Schlappi H, Schlappi M, Ireland TV. Reflex control of the spine and posture: a review of the literature from a chiropractic perspective. Chiropr Osteopat. 2005 Aug 9;13:16.
- Gieysztor E, Pecuch A, Kowal M, Borowicz W, Paprocka-Borowicz M. Pelvic Symmetry Is Influenced by Asymmetrical Tonic Neck Reflex during Young Children's Gait. Int J Environ Res Public Health. 2020 Jul 2;17(13):4759.
- Reynolds JS, Blum D, Gdowski GT. Reweighting sensory signals to maintain head stability: adaptive properties of the cervicocollic reflex. J Neurophysiol. 2008 Jun;99(6):3123-35.
- Wang M, Yu J, Li H, Zhao C, Li Y, Yang X. Development of the children's primitive reflex integration assessment scale. Front Psychol. 2025 Jan 22;16:1495990.
- Parhizi B, Barss TS and Mushahwar VK (2021) Simultaneous Cervical and Lumbar Spinal Cord Stimulation Induces Facilitation of Both Spinal and Corticospinal Circuitry in Humans. Front. Neurosci. 15:615103.
- Blum CL, Lovett Brothers: The Relationship Between the Cervical and Lumbar Vertebra. The Journal of Vertebral Subluxation Research. Apr 2004; 6(1): 1-3.
- Blum C. (2015). R + C Factors and Sacro Occipital Technique Orthopedic Blocking: a pilot study using pre and post VAS assessment. The Journal of the Canadian Chiropractic Association. 59. 134-42.
- Kondratiev A, Smetankina N, Staude V. Biomechanical Analysis of Stress–Strain Distribution in the Lumbar Spine–Sacrum–Pelvis System with Emphasis on Sacroiliac Joint Dysfunction. Prosthesis. 2025; 7(1):4.
- Peng B, Yang L, Li Y, Liu T, Liu Y. Cervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative Review. Pain Ther. 2021 Jun;10(1):143-164.
- Getzoff H, Blum CL. A study of the nature of SOT occipital line fibres: A retrospective case series of 65 patients. Asia-Pac Chiropr J. 2025;5.4.
- Germann AM, Kashyap V. Anatomy, Head and Neck, Occipital Bone, Artery, Vein, and Nerve. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-.
- Hack GD, Koritzer RT, Robinson WL, Hallgren REC, Greenman PE. Anatomical relation between the rectus capitis posterior minor muscle and dura mater. Spine. Dec 1995;20(23): 2484-6.
- Scali F, Marsili ES, Pontell ME. Anatomical connection between the rectus capitis posterior major and the dura mater. Spine (Phila Pa 1976). 2011 Dec 1;36(25):E1612-4.
- Pontell ME, Scali F, Enix DE, Battaglia PJ, Marshall E. Histological examination of the human obliquus capitis inferior myodural bridge. Ann Anat. 2013 Dec;195(6):522-6.
- Li C, Yue C, Liu ZC, Gong J, Wei XS, Yang H, Gilmore C, Yu SB, Hack GD, Sui HJ. The relationship between myodural bridges, hyperplasia of the suboccipital musculature, and intracranial pressure. PLoS One. 2022 Sep 2;17(9):e0273193.
- Enix DE, Scali F, Pontell ME. The cervical myodural bridge, a review of literature and clinical implications. J Can Chiropr Assoc. 2014 Jun;58(2):184-92.
- Mitchell B, Humphreys BK, O’Sullivan E. Attachment of the ligamentum nuchae to cervical posterior spinal dura and the lateral part of the occipital bone. Journal of Manipulative and Physiological Therapeutics. Mar/Apr 1998; 21(3): 145-8.
- Shinomiya K, Dawson J, Spengler DM, Konrad P, Blumenkopf. An analysis of the posterior epidural ligament role on the cervical spinal cord. Spine. Sep 1996;21(18):2081-8.
- Bashline SD, Bilott JR, Ellis JP. Meningovertebral ligaments and their putative significance in low back pain. Journal of Manipulative and Physiological Therapeutics. Nov/Dec 1996; 19(9): 592-6.
- Barbaix E, Girardin MD, Hoppner JP, Van Roy P, Claris JP. Anterior sacrodural attachments Trolard’s ligaments revisited. Manual Therapy. Mar 2000; 1(2):88-91.
- Gaddam SS, Santhi V, Babu S, Chacko G, Baddukonda RA, Rajshekhar V. Gross and microscopic study of the filum terminale: does the filum contain functional neural elements? J Neurosurg Pediatr. 2012 Jan;9(1):86-92.
- Martini ML, Neifert SN, Chapman EK, Mroz TE, Rasouli JJ. Cervical Spine Alignment in the Sagittal Axis: A Review of the Best Validated Measures in Clinical Practice. Global Spine J. 2021 Oct;11(8):1307-1312.
- Dean NA, Mitchell BS. Anatomic relation between the nuchal ligament (ligamentum nuchae) and the spinal dura mater in the craniocervical region. Clin Anat. 2002 May;15(3):182-5.
- Kahkeshani K, Ward PJ. Connection between the spinal dura mater and suboccipital musculature: evidence for the myodural bridge and a route for its dissection--a review. Clin Anat. 2012 May;25(4):415-22.
- Getzoff H. Sacro Occipital Technique (SOT): A Systems Driven Method of Chiropractic. Asia-Pac Chiropr J. 2024;4.4.
- Getzoff H. The Atlas Vertebrae and its role in the function of the Sacro Occipital Technique (SOT) Categories. Asia-Pac Chiropr J. 2025;5.4.
AU: Oscar Bacino, BSc (Physio); MSc (Psych); B Chiro; Cert (Gonstead); Cert (Extremity); GCSS; MNZCA. Private practice, Dannevirke, New Zealand. e: oscar@oscarbacino.com
- Outline core Stoic philosophical principles, with attention to their practical, way-of-life orientation, (7-12)
- Summarise key elements of classic Chiropractic philosophy as articulated by DD Palmer, BJ Palmer, Stephenson, Gonstead and later authors, (16-21)
- Explore conceptual parallels and differences between Stoic and Chiropractic worldviews, and to
- Analyse how Stoic way of life might be integrated with a contemporary Chiropractic way of life to clarify professional identity and add value in modern health care.
- meditative reflection,
- journaling,
- pre-meditation of potential difficulties,
- review of one's actions,
- voluntary simplicity, and
- conscious rehearsal of appropriate response to adversity. (9, 14, 15)
- The universe is ordered by a ‘Universal Intelligence’ that expresses itself through ‘innate intelligence’ in living organisms,
- Health is the unobstructed expression of this innate organising principle; disease arises from interference (often mechanical) with its transmission, and
- The Chiropractor’s role is specific, principled adjustment-not general manipulation or symptomatic treatment.
- What is under control:
- The clinical quality of each adjustment.
- The honesty, proportionality and evidence-basis of their claims.
- Their willingness to engage respectfully in intra, and interprofessional dialogue.
- Their commitment to continual learning and self-scrutiny.
- What is not fully under their control:
- The actions of other chiropractors.
- Media narratives and social media attacks.
- Policy decisions by insurers, regulators, or governments.
- If subluxation is retained, it should be as a carefully defined, testable concept consistent with contemporary neurobiology and clinical evidence, (19, 22-24)
- If empirical support for strong causal claims is lacking, the virtuous response is to moderate language, acknowledge uncertainty, and avoid over-promising outcomes, and
- Either way, clinging to subluxation primarily as a badge of tribal belonging fails the Stoic test of aligning belief with reason and evidence. (7, 9, 13)
- Morning intention-setting: Briefly reviewing the day’s schedule and pre-meditating likely challenges: a sceptical patient, a complex case, a confrontational colleague. The practitioner rehearses responding with patience, clarity, and professionalism.
- Evening reflections: Writing a short journal note on three questions:
- What did I do well today in line with my values as a Chiropractor?
- Where did I fall short (e.g. rushed, over-stated, reacted defensively)?
- What can I do differently tomorrow?
- Voluntary simplicity: Periodically choosing to practise contentment with fewer external rewards, seeing criticism, financial stress or uncertainty as training in prioritising intrinsic over extrinsic goods.
- Explaining spinal and nervous-system concepts in biologically plausible, jargon-free language, avoiding deterministic promises
- Framing the adjustment not as a magical intervention but as a once tool among others (movement, load management, sleep, stress reduction) just to name a few, to help the body adapt and function more effectively
- Acknowledge uncertainty: ‘Based on the best evidence and my experience, this is how I think I can help; here are the limits of what I know’.
- What set of beliefs and practices best serves patient’s long-term interests and the common good?
- How can chiropractors who differ on metaphysical or scope-of-practice questions still collaborate on shared commitments to honesty, clinical competence and respect for evidence?
- Guardians of spine and movement health with a nervous-system focus: Building on Nelson’s and Schneider’s models, (22, 23) Chiropractors can present themselves as primary-contact practitioners specialising in conservative, hands-on management of spine-related and neuro-musculoskeletal problems, guided by evidence where it exists and by transparent reasoning where it does not.
- Clinicians who integrate technical excellence with character excellence: A Stoic-Chiropractic way of life highlights the virtues of attentiveness, patience, courage in discussing uncertainty, and justice in avoiding over-servicing or under-referral. This can distinguish Chiropractors in systems that increasingly value relational continuity and trust.
- Educators of embodied self-care. Many Chiropractic practices already incorporate lifestyle advice around posture, movement, stress, and nutrition. A Stoic framework can deepen this by explicitly coaching patients in distinguishing controllable and uncontrollable factors, focusing on purposeful actions rather than catastrophising, and adopting realistic, value-consistent health goals. (13-15, 22, 23)
- Participants in a broader evidence-informed, virtue-based spine-care community. Rather than defining identity in opposition to medicine or physiotherapy, Chiropractors can align with other professions around shared commitments to patient-centred, evidence-informed care while still maintaining specific techniques and traditions where these are shown to be safe and effective (1-3, 22, 23).
- Qualitative studies of chiropractors who explicitly engage with Stoic practices and their impact on burnout, resilience and ethical decision-making.
- Educational interventions introducing Stoic concepts into chiropractic curricula and examining effects on students handling of identity tensions (4-6).
- Philosophical work critically comparing Stoic concepts of nature and reason with contemporary biological and neurophysiological models relevant to spinal care (19, 22, 23).
Also by this author
Bacino O. The healing touch: Where ancient wisdom meets modern technology in Chiropractic care. Asia-Pac Chiropr J. 2026;6.3. www.apcj.net/papers-issue-6-3/#BacinoHealingTouch
References
- Meeker WC, Haldeman S. Chiropractic: a profession at the crossroads of mainstream and alternative medicine. Ann Intern Med. 2002;136(3):216–227.
- Villanueva‑Russell Y. Caught in the crosshairs: identity and cultural authority within chiropractic. Soc Sci Med. 2011;72(11):1826–1837. DOI 10.1016/j.socscimed.2011.03.038.
- Leboeuf‑Yde C, Innes SI, Young KJ, Kawchuk GN, Hartvigsen J. Chiropractic, one big unhappy family: better together or apart? Chiropr Man Therap. 2019;27:4. DOI 10.1186/s12998-018-0221-z. Available from: Chiropractic & Manual Therapies.
- Gliedt JA, Hawk C, Anderson M, et al. Chiropractic identity, role and future: a survey of North American chiropractic students. Chiropr Man Therap. 2015;23:4. DOI 10.1186/s12998-014-0048-1. Available from: Chiropractic & Manual Therapies.
- de Luca KE, Gliedt JA, Fernandez M, Kawchuk G, Swain MS. The identity, role, setting, and future of chiropractic practice: a survey of Australian and New Zealand chiropractic students. J Chiropr Educ. 2018;32(2):115–125. DOI 10.7899/JCE-17-24. Available from: PubMed Central.
- McGregor M, Puhl AA, Reinhart C, Injeyan HS, Soave D. Differentiating intraprofessional attitudes toward paradigms in health care delivery among chiropractic factions: results from a randomly sampled survey. BMC Complement Altern Med. 2014;14:51. DOI 10.1186/1472-6882-14-51.
- Sellars J. Stoicism. Berkeley, CA: University of California Press; 2006.
- Long AA, Sedley DN. The Hellenistic Philosophers. Vol. 1. Cambridge: Cambridge University Press; 1987.
- Hadot P. Philosophy as a Way of Life: Spiritual Exercises from Socrates to Foucault. Chase M, translator. Oxford: Blackwell; 1995.
- Epictetus. Discourses and Selected Writings. Dobbin R, translator. London: Penguin; 2008.
- Seneca. Letters from a Stoic. Campbell R, translator. London: Penguin; 1969.
- Aurelius M. Meditations. Hays G, translator. New York: Modern Library; 2002.
- Robertson D. The Philosophy of Cognitive Behavioural Therapy (CBT): Stoic Philosophy as Rational and Cognitive Psychotherapy. London: Karnac Books; 2010.
- Irvine WB. A Guide to the Good Life: The Ancient Art of Stoic Joy. Oxford: Oxford University Press; 2009.
- Pigliucci M. How to Be a Stoic: Using Ancient Philosophy to Live a Modern Life. New York: Basic Books; 2017.
- Palmer DD. The Chiropractor's Adjuster: The Science, Art and Philosophy of Chiropractic. Portland, OR: Portland Printing House; 1910.
- Palmer BJ. The Bigness of the Fellow Within. Davenport, IA: Palmer School of Chiropractic; 1949.
- Stephenson RW. Chiropractic Textbook. Davenport, IA: Palmer School of Chiropractic; 1927.
- Gatterman MI, editor. Foundations of Chiropractic: Subluxation. 2nd ed. St Louis, MO: Mosby; 2005.
- Cooperstein R, Gleberzon BJ. Technique Systems in Chiropractic. New York: Churchill Livingstone; 2004.
- Plaugher G. Textbook of Clinical Chiropractic: A Specific Biomechanical Approach. Baltimore, MD: Williams & Wilkins; 1993.
- Nelson CF, Lawrence DJ, Triano JJ, et al. Chiropractic as spine care: a model for the profession. Chiropr Osteopat. 2005;13:9. DOI 10.1186/1746-1340-13-9.
- Schneider MJ, Murphy DR, Hartvigsen J. Spine care as a framework for the chiropractic identity. J Chiropr Humanit. 2016;23(1):14–21. DOI 10.1016/j.echu.2016.09.004.
- Hart J. Analysis and adjustment of vertebral subluxation as a separate and distinct identity for the chiropractic profession: a commentary. J Chiropr Humanit. 2016;23(1):46–52. DOI 10.1016/j.echu.2016.09.002.
AU: Richard M. Burger, DC, CCSP, DIBAK. Clinic Director, San Diego Sports Medicine Chiropractic Clinic, San Diego CA. e: rmbdc@earthlink.net
Narrative: The buccinator muscle may be a significant factor in cranial and temporomandibular joint involvement with a reactive muscle type of relationship with the masseter. Frequently there is an associated hypertonic temporalis muscle. The buccinator may be challenged with stretch by filling both cheeks as full as possible with air. Lateralizing the full cheek gives indication of the side of involvement; rarely bilateral. Confirmation by therapy localization is possible. Treatment is by approximating the muscle belly. This procedure should be a screening test in the evaluation of the stomatognathic system. For patient management in difficult cases the patient can be instructed to maximally expand the cheeks with air and hold the expansion for 30 seconds to two minutes, resulting in reduction of jaw muscle tension and symptoms.
Cite: Burger RM. The Four Realms and Purpose: Setting standards ‘above the line’. Asia-Pac Chiropr J. 2026;7.1. https://www.apcj.site/BurgerBuccinator.pdf
Bibliography
Goodheart G H Jr. Applied Kinesiology Research Tape Number 28. Grosse Pointe Woods, MI: Privately published; 1976. Transcribed by: Diener MS. Park City, UT. 1984:28-1,28-2.
Hollinshead W H. Textbook of Anatomy. 3rd ed. Hagerstown, Maryland: Harper & Row, Publishers; 1974:816.
Platzer W. Color Atlas and Textbook of Human Anatomy in 3 Volumes. Vol 1. Chicago, Ill: Year Book Medical Publishers; 1978:308.
Walther DS. Applied Kinesiology Volume II--Head, Neck, and Jaw Pain and Dysfunction--The Stomatognathic System. Pueblo, Co: Systems DC; 1983:101.
Goodheart G H Jr. Applied Kinesiology Research Tape Number 31. Grosse Pointe Woods, MI: Privately published; 1976. Transcribed by: Diener MS. Park City, UT. 1984:31-2.
Walther DS. Applied Kinesiology Volume II--Head, Neck, and Jaw Pain and Dysfunction--The Stomatognathic System. Pueblo, Co: Systems DC; 1983:251.
Blanton PL et al. Cited by: Walther DS. Applied Kinesiology Volume II--Head, Neck, and Jaw Pain and Dysfunction--The Stomatognathic System. Pueblo, Co: Systems DC; 1983:251.
Goodheart G H Jr. Applied Kinesiology Research Tape Number 31. Grosse Pointe Woods, MI: Privately published; 1976. Transcribed by: Diener MS. Park City, UT. 1984:31-2.
AU: Philip Maffetone, DC. Retired practitioner, health-fitness writer, researcher, songwriter. e: Phil@MaffetoneMusic.com
Cite: Maffetone P. Health Profilers: Is that a reflection in the Mirror Neurons? Asia-Pac Chiropr J. 2026;7.1. https://www.apcj.site/MaffetoneReflection.pdf
Clinical evidence as case reports

Sacro Occipital Technique (SOT) and Gastro-esophageal Reflux Disease (GERD): A Case Report
This paper studies a successful outcome (a reduction of the signs and symptoms) of a patient experiencing the effects of GERD that was treated by SOT Chiropractic methods.
Narrative: The objective of this paper is to study the Sacro Occipital Technique (SOT) Chiropractic care of a female patient experiencing a chronic sore throat, persistent heartburn and at times difficulty swallowing.
Additionally, she reported various digestive symptoms such as abdominal cramping and bloating along with some upper abdominal pain.
The patient had been experiencing these signs and symptoms for approximately four years, during which she was medically diagnosed with Gastroesophageal Reflux Disease (GERD) and has been receiving medical treatment for this condition.
Author note: It is my hope that this case report “will serve as a mini tutorial for others” (1) not only those caring for patients with Gerd but also for chiropractors adjusting patients with other organ and spinal related problems.
Indexing Terms: Sacro Occipital Technique (SOT); MB DeJarnette DC; Occipital Fibers; Chiropractic Manipulative Reflex Technique (CMRT); Gastroesophageal Reflux Disease (GERD).
Cite:Getzoff H. Sacro Occipital Technique (SOT): Gastroesophageal Reflux Disease (GERD) ~ A Case Report. Asia-Pac Chiropr J. 2026;7.1. https://www.apcj.site/GetzoffGERD.pdf
Introduction
GERD is most often caused by changes in the barrier tissue between the stomach and the esophagus, known as the lower esophageal sphincter (LES). ‘The LES typically keeps the top of the stomach closed, preventing the acid content of the stomach from ascending back up into the esophagus’, (3) where it can cause burning, inflammation and damage to the sensitive esophageal tissue. ‘GERD is a condition where the acid in the stomach washes back, ascending into the esophagus’. (4) ‘Since the esophagus lacks the protective mucosal lining of the stomach it is easily irritated by the digestive juices’. (5)
The medical diagnosis is usually based on the patient’s presentation and symptomatology. (3, 4) The usual medical treatment for Gerd includes lifestyle modifications, medication and possibly surgery. Initial medical treatment often involves a protein pump inhibitor, such as Omeprazole (Prilosec). ‘Omeprazole is used to treat certain conditions where there is too much acid in the stomach. It is used to treat gastric and duodenal ulcers, erosive esophagitis and gastroesophageal reflux disease (GERD)’. (4)
SOT Chiropractic
SOT was founded and developed by Dr MB DeJarnette. (4, 6, 8) We honour DeJarnette for his 70 plus years of extensive research and study all presented and explained in detail in his yearly seminar notes, numerous additional writings and his yearly conferences. SOT is based on the identification, via SOT indicators (specific tests and observations), of the state of function of three primary systems of the body, known as categories, and the SOT adjustments considered necessary to improve their function. The three SOT categories are each clinically definable but at the same time interrelated. (26,27)
- Category one pertains to the Primary Cranial Sacral Respiratory Mechanism (PCSRM). The term respiratory refers to the intrinsic motion of the cranial and sacral components of the PCSRM which facilitates tension of the dura and the subsequent circulation of cerebral spinal fluid (CSF). This process is essential for the protection and the nourishment of the central nervous system (CNS). (4, 26, 33) The SOT indicator Heel Tension serves as the chief indicator for category one being the category most in need of adjustment. (4, 26, 33) Heel tension represents a deficiency in the respiratory function of the sacrum and the inability of the atlas vertebrae to respond sufficiently to the needs of the PCSRM. (4, 6, 31)
- Category two refers to ligamentous sacroiliac weight-bearing instability, resulting from the accumulation of instability throughout the entire structural system, inclusive of the sutures of the cranium.(4, 6, 26) The SOT Arm/fossae test monitors the nervous system’s sensory/motor response to the instability of the weight-bearing portion of the sacroiliac joint and if indicated, category two is the category most in need of adjustment, superseding heel tension if present.(4, 26, 28)
- Category Three pertains to lumbar subluxations, lumbar disc lesions and the condition of the sciatic nerve, along with functionally necessary adaptations primarily of the piriformis muscle and possibly of the psoas muscle and the upper cervical region. The primary indicator for category three is the Step Out Toe OUT (SOTO) test which assesses the function of the piriformis muscle in relationship to a lumbar disc lesion or a potential entrapment of the sciatic nerve. (6, 7, 33) When SOTO is present and the arm fossae test is negative category three is the category of choice.
Chart #1: Two portions of the sacroiliac joint

SOT Categories=" A" Model of Function + A State of Dysfunction + A Method of Adjustment
Case Report
Initial Office Visit
History
A 43-year-old woman of average weight presented in my office experiencing a sore throat, heartburn, difficulty swallowing and various digestive symptoms such as cramping, bloating and some upper abdominal pain. She also reported left-sided neck pain with bilateral upper back pain (in the mid thoracic area), seasonal allergy symptoms and periods of anxiety that she felt were associated with her GERD symptoms. This was her first visit to a Chiropractor. She was referred by her mother who at the time was a patient in my office.
The patient was regularly taking Omeprazole (Prilosec) for the past two months and Xanax for clinical anxiety along with over-the-counter allergy medication as needed, all prescribed by her treating medical specialist. The patient consumed a gluten free and dairy free diet. All symptoms presented were chronic, more pronounced and inhibitory over the last four years, even with the diet modifications and medical intervention. An ultrasound examination was performed four months prior to her initial visit to the office but revealed no abnormalities.
The patient expressed a deep concern about her inability to fulfil her role as a mother (two young children) and as a part-time occupational therapist, all due to her symptoms.
Examination
An examination with an emphasis on SOT methods of analysis was performed at the initial visit. (4, 6, 33)
While standing in front of a plumb line, on a fixed foot plate, with her eyes closed and the examiner standing behind her the following was observed. The patient exhibited lateral motion in excess, along with a dominant left thoracic /first rib joint swelling with greater movement than the right, indicative of the body struggling to gain stability. (4,6,33) The patient’s spine curved to the left, initiated at the lower lumbar spine, while her right ear was inferior when compared to her left ear.
In the seated position, performing cervical ranges of motion, the patient exhibited limitations in both left lateral flexion (40 degrees) and right rotation (80degrees). (6,7,26)
In the prone position a line two area 3 occipital fibre was detected on the left, coupled with a spinous process compression subluxation of thoracic 5/6. Occipital fibres, line 2 are considered to be defensive, reacting in a reflex pattern associated with a spinal subluxation and a related organ. (2,16,32). ‘Spinal postural accommodations were mediated through the visual and vestibular righting reflexes and reflected in related specific suboccipital muscle fibre contracture (occipital fibres).’(2) ‘Occipital fibre technique locates and identifies subluxations and can be utilised to help identify specific viscerosomatic/somatovisceral reflex organ disorders, incorporating specific soft tissue visceral and somatic therapies’, (2,11) referred to as Chiropractic Manipulative Reflex Technique (CMRT).
Occipital fibre therapy can facilitate the management of dis-ease while at the same time providing a philosophy of care. (11, 13)
A line two occipital fibre, area three, in conjunction with a thoracic 5/6 subluxation identifies a gastric dysfunctional problem. ‘The resulting system designates the horizontal vector as lines, the vertical vector as areas’. (11)
Chart #2: Line Two occipital fibres and their related vertebrae/organ
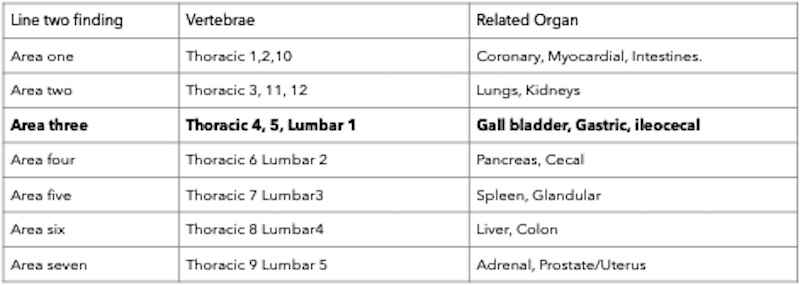
In the supine position there was a right leg deficiency with a left lower arm/fossa finding. The arm/fossae test denotes the response of the arm when placed in a specific upright position and pulled on command while placing simultaneous pressure on specific portions of the inguinal ligament. The inguinal ligament receptor system responds to disturbances at the weight-bearing portion of the sacroiliac joint. Thus, the arm/fossae test accesses the stability of the weight-bearing portion of the sacroiliac joint, which is primary in identifying an SOT category two in need of adjustment. (6 ,7, 26) A leg length discrepancy in conjunction with the arm/fossae finding determines the need for blocks and where to place them.
Also identified in the supine position were cranial findings involving the right maxillary/malar suture resulting from underdevelopment of the right mid facial bones, primarily the malar. (8, 29) Cranial sutural dysfunction often initiates disturbances in the head righting reflexes that can create imbalances and instability throughout the body. (2, 29, 31)
All of these findings were interrelated, systems oriented (category two) (27, 28) and addressed the patient’s concerns. Based on these findings, most specifically the occipital fibre findings line two, area three, thoracic five/six as well as the patient’s established commitment to lifestyle modifications, it was my belief that SOT Chiropractic would provide effective care and necessary improvement.
Chart # 3: SOT primary category indicators
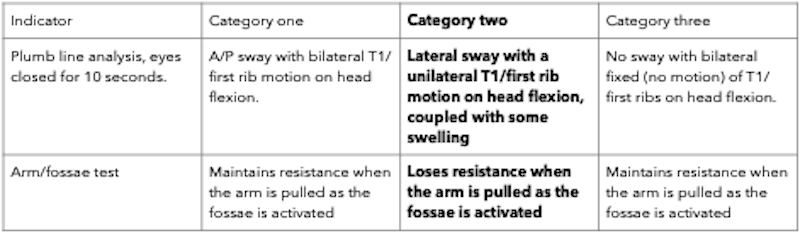
SOT category two adjusting procedures were implemented.
- Category two supine blocks (6, 7, 28)
- Category two basic 2 cranial adjustment (6, 7, 28)
- Retesting of arm/fossae, leading to the removal of the blocks (6, 26, 28)
- SOT cervical stairstep and figure eight adjusting (12, 26)
- Category two sutural adjusting focused on the right maxillary/malar suture. (8, 14, 29)
As previously discussed incorporated into the SOT category two adjusting method was the occipital fibre line two technique (stimulation of line two area 3) adjustment of thoracic 5/6 for inferior spinous process and CMRT of thoracic 5 soft tissue indicators.(2, 16, 25) All examination findings were retested at each office visit and were recorded accordingly. (30)
Nothing in SOT is done without a reason and no action is complete until it is re-evaluated, all guided by indicators’. (26, 33)
- Blocks were utilised on 11 of the 13 office visits indicated by the arm/fossae test
- Basic 2 cranial adjusting was utilised when blocking was utilised (5, 28)
- Cervical stairstep, figure 8 adjusting was utilised at each adjustment even though sitting cervical findings, lateral flexion, right rotation, were normal after the fifth adjustment
- Cranial sutural adjusting continued throughout the 13 adjustments based on the cranial findings of the day, right head position, limited cranial ranges of motion on the right maxillary/malar suture compared to the left and the presence of underdevelopment in the facial structures on the right side of the face. (29 ) A 5-step adjusting procedure was utilised focused in the right maxillary/malar suture. (29)
- The occipital fibre, line 2 area 3, thoracic 5/6 interspinous space and the thoracic 5 soft tissue reflexes (CMRT) were utilised throughout the 13 adjustments. (2, 16) Occipital line two fibres and their related vertebral subluxations are considered defensive and therefore remain throughout care. (2, 16, 32) ‘The occipital fibre is purely defensive and the result of other happenings. It is not causative, as long as the fibre responds, the body’s defense is normal’. (7)
DeJarnette’s premise of treatment beginning with the occipital fibre neutralisation, vertebral adjustment and reflex manipulations was that there was an imbalance between the organ, the spine and within the autonomic nervous system. (2)
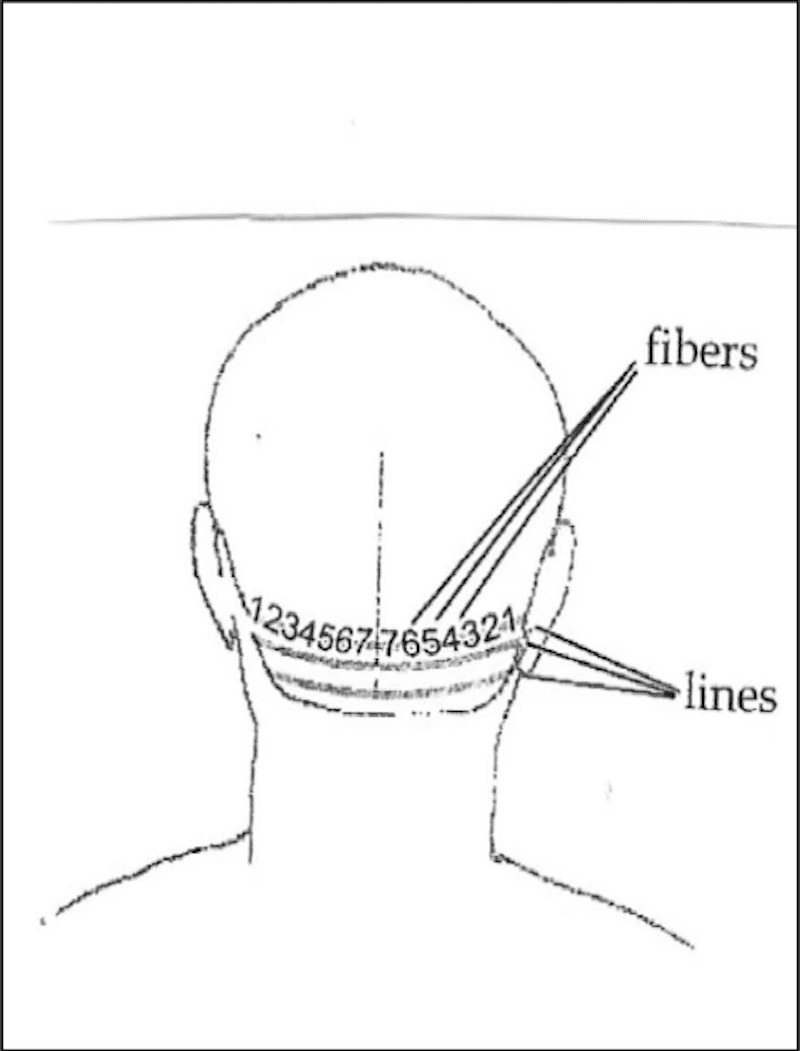
Outcomes
Discussion
Timeline
Initial visit, 13 adjustments over 2 months, followed by one adjustment approximately every 3 to 4 weeks for 16 months, and then mainly monthly adjustments over 4½ years.
Plumbline Findings
Less lateral sway, less tenderness and swelling of T1/first rib throughout the 4½ years of care, all indicative of the weight-bearing system regaining stability. (4,6,26)
History of the day
At each office visit, I asked the patient, ‘How are you feeling?’ and recorded her reply in my daily notes, as per my recording system outlined in my paper previously published in this journal. (30) Her symptoms related to GERD gradually diminished, leading her to discontinue Omeprazole and instead use a natural digestive enzyme with her evening meal. There were no reported episodes (flare up of symptoms) during her care, but she did report right jaw pain and was referred to an orthodontist for care. She did continue the usage of Xanax but did express that she was happily working her preferred 20-hour shift as an occupational therapist at a nearby rehabilitation hospital.
Arm/fossae testing for category two blocks
The arm fossae test was initially positive, left leg deficiency with a left upper fossa response, indicating the need for blocks. The arm/fossae test was negative overtime indicating no need for blocks. This indicated progress, as the functioning of structures improved and the weight-bearing aspect of the sacroiliac joint achieved greater stability. (26, 28)
Cervical ROM
Improved as of the fifth adjustment and maintained normal function throughout her care. Nevertheless, cervical range of motion was checked at each adjustment and stairstep and figure 8 adjusting was continually utilised to maintain function. The patient continued to comply with her home-care instructions. (6, 7, 33)
Cranial Sutural
The cranial range of motion for the malar (zygoma) remained present throughout care but was considered by both me and the patient to be less restricted and less tender when tested. Cranial adjustments: maxillary rotation, straddle and sutural release, in conjunction with malar lift were utilised to expand the maxilla/malar sutural contraction. (13, 14, 15) Sutural expansion is considered functional while sutural contraction is considered dysfunctional. Head tilt was improved, often not present, cranial adjustments remained addressing the facial underdevelopment of the right malar and her history of right jaw pain.
Occipital Fibre Line 2 Technique
Line 2 fibres serve a defensive role, so treatment aims to enhance function in both the vertebra and viscera, as well as to prevent these areas from becoming pathological (line 3). (2, 3) In this case, improved function is reflected by the patient’s reported history for the day, less tenderness and sensitivity and notably decreased tenderness along the line 2 fibres, the spine and CMRT tissues. Clinically this is found to be associated with improvement of gastric function.
The Occipital Fibre Line 2 technique consists of the following steps
- Stimulate the line two fibre (2)
- Adjust the T5 spinous process in a superior direction (2)
- Using one hand, rub the web between the left index finger and thumb while gently massaging the area between the patient’s umbilicus and xiphoid process with the other hand (2)
- Simultaneously hold the trapezius region of the shoulder and the area above the umbilicus, look for relaxation in the contacted tissues. (2)
Conclusion
As previously stated, the objective of this case report is to provide an educational resource regarding the SOT method of Chiropractic care and to illustrate its application in managing an organ-related condition, following the JBI (Joanna Briggs Institute) model of Evidence-Based Healthcare for case reporting, as described by Cuthbert and Ebrall. (1)
The JBI model is a cycle that fosters the synthesis of evidence and then its transfer to where it is needed and its subsequent implementation. (1) This study seeks to adhere to the guidelines of the JBI model by presenting thorough contextual information and offering a comprehensive evaluation of both the process and outcomes associated with the SOT methods of Chiropractic care.
Since the symptoms and the examination findings that determined the diagnosis have been significantly reduced it appears that the interventions as presented in this single case study were successful. She subsequently referred both her husband and son to my office for care.
I recognise Dr DeJarnette for his dedicated research and tireless work in advancing the understanding of the connection between bodily structure and organ systems, leading to the discovery of occipital fibres, specific vertebral adjustments, and the Chiropractic manipulative reflex technique.
References
- Cuthbert S, Ebrall P. The Contemporary Role of the Case Report in Evidence Generation for the Discipline of Chiropractic. Asia-Pacific Chiropr J.2024; 5.1.
- BlumCL. Chiropractic Manipulative Reflex Technique. Chiropractic in the Field of Non-Musculoskeletal Care, Published Amazon. Com. July 2024:
- DeVault KR, Castell DO, American College of Gastroenterology. Updated guidelines for the diagnosis and treatment of gastroesophageal reflux disease. Am J Gastorenterol.2005 Jan;100(1): 190-200.
- Mayo Clinic Online-Gerd. www.mayoclinic.org/disease-conditions/gerd/basics/definition/con-con-2002520.
- John Hopkins Symptoms and remedies, Medical Editor, Simeon Margolis, MD, PHD. Publisher Random House 1995. 446-7.
- DeJarnette MB. Sacro Occipital Technique, Nebraska City, NE: Self-Published, 1980:4, 207, 306.
- DeJarnette MB. Sacro Occipital Technique, Nebraska City NE: Self-Published, 1984: 51,75,101,116-42.
- DeJarnette Mb. Cranial Technique, Nebraska City, Ne:Self-Published,1979-1980:14.
- Mootz R, Jameson S, Menke M, Inter and Intra-Rater Reliability of Occipital Fiber Palpation. Proceedings of the fifth Annual Conservative Health Science Research Conference. Oct. 1986: 37-9.
- Hesse N. Occipital Fiber Physiology and line 3 therapy. Sacro Occipital Research Society International, Technical report. March 1998; 10 (10.
- Evans AC. Yelverton C. The Validity and Specificity of the Arm/Fossae test. World Federation of Chiropractic’s 12th Biennial Congress, South Africa. April 10-13, 2013.
- Blum CL. Sacro Occipital Technique (SOT): The Cervical Stairstep Adjustment. A Position Statement. Sacro Occipital Technique Organization- Usa: Sparta, North Carolina.2010.
- Getzoff IH. Analysis of the Cranium Through the use of Cranial Ranges of Motion. Sacr Occipital Research Society International, Technical Report. Nov. 1991; 3 (4).
- Getzoff IH. A Practical Guide to Cranial Adjusting. Weidner and Sons Publishing 1996: 20-1,29, 33-36.
- Getzoff IH. The Role of the Malar Bone in Cranial Function. Sacro Occipital Research Society International, Technical Report. January 1990 2 (1).
- DeJarnette MB. Chiropractic Manipulative Reflex Technique. Self-Published: Nebraska City NE. 1966: 27-33.
- Dangerfield A. CMRT. Chiropractic Manipulative Reflex Technique. Sacro Occipital Research society International, Technical Report. April 1995; 7 (1).
- Guyton A, Hall J. Human Physiology and Mechanisms of Disease. Sixth Edition; W.B. Saunders Co. 1997. 515-16, 363-364, 463-465, 500.
- Morningstar MW, Pettibon BR, Schlappi H, Schlappi M, Ireland TV. Reflex Control of the Spine and Posture: A review of the literature from a chiropractic perspective. Chiropr. Osteopat. 2005 Aug 9;13;16.
- Fink M, Wahling K, Stiesch- Scholtz M, Tschernitschek H.. The Functional Relationship Between the Craniomandibular System, Cervical Spine and the Sacroiliac Joint. A Preliminary Investigation. Cranio 2003.July 21; (3); 202-8.
- Klingensmith RD, Blum CL, Chiropractic Manipulative Reflex Technique; treatment for Gerd of a 3-year-old male: A Case Report. International Chiropractic Pediatric Association: Pediatric research Conference: Wellness Conference, Washington DC, October 2010.
- Butafava J, Dal bello F, Blum CL. The Alterations of Dyspeptic Signs and Symptoms of Patients with Gastritis Following Chiropractic Treatment: A small randomized controlled study. J Chiropr. ED. Spring 2012, 24 (1) :85.
- Dal Bello F, Dal Bello V, Raupp JM, Santos LN. Alterations of dyspeptic signs and symptoms in patients presenting with gastroesophageal reflux disease following chiropractic treatment. J Chiropr. Edu. 2010 24(10:124.
- Mitchell GA, Blum CL. Sacro Occipital Technique Treatment of Hiatal Hernia Presentation: a Case Report. J Chiropr.Edu. Spring 2011, 25 (1): 114.
- Blum Cl. Chiropractic Manipulative Reflex Technique. Sacro Occipital technique Organization-USA: Sparta, North Carolina. 2014. b
- Getzoff IH.A Critical Approach to Learning the Operating Principles of Sacro Occipital Technique (SOT) Chiropractic. Pub. Asia Pacific Chiropr. J.2023,3,4. Online.
- Getzoff IH. Sacro Occipital Technique: A Systems Driven Method of Chiropractic: Pub. Asia Pacific Chiropr. J.2024,4,4. Online.
- Getzoff IH. Sacro Occipital Technique. Category Two Systems Integration. Pub. Asia Pacific Chiropractic Journal. 2024, 5,1. Online.
- Getzoff IH. A Primary Cranial Analysis and Adjusting Method for all three SOT categories: A retrospective Study of 85 Patients. Pub. Asia Pacific Chiropr J. 2023,4,4. Online.
- Getzoff, IH. Sacro Occipital Technique: Documentation and Recording System . Pub. Asia Pacific Chiropr. J. 2024; 5,2. Online.
- Getzoff IH. The Atlas Vertebrae and its Role in the Function of the Sacro Occipital Technique Categories, Pub. Asia Pacific Chiropractic Journal, 2025,5,4. Online.
- Getzoff IH, Blum CL. A Study of the Nature of Sacro Occipital Technique: Occipital Line Fibers- A Retrospective Case Series of 65 Patients. Pub. Asia Pacific Chiropr. J 2025, 5,4. Online.
- Getzoff IH. Sacro Occipital Technique (SOT) Indicators: Accessing Problems and developing Strategies. Asia Pacific Chiropr. J. 2026; 6,3. Online.
Also by this author
In this Journal
- Getzoff H. Sacro Occipital Technique (SOT) Indicators: Accessing Problems and Developing Strategies. Asia-Pac Chiropr J. 2026;6.3. apcj.net/Papers-Issue-6-3/#GetzoffSOTStrategies
- Getzoff H. A Critical Approach for learning the Operating Principles of Sacro Occipital Technique (SOT) Chiropractic. Asia-Pac Chiropr. J. 2023;3,4. http://apcj.net/Papers-Issue-3-4/#GetzoffSOTPrinciples
- Getzoff H. Sacro Occipital Technique (SOT). Category Three: Predictability of Outcomes. Asia-Pac Chiropr. J 2024;4.3. http://apcj.net/Papers-Issue-4-3/#GetzoffSOTCat3
- Getzoff IH. The Sitting Disc Technique and the Relationship to the Straight Leg Raise Test: A Retrospective Case Series of thirty Patients. Asia Pac. Chiropr. J. 2020; 1,2. https://apcj.rocketsparkau.com/sitting-disc-and-slr--getzoff/
- Getzoff H. Anterior Thoracic adjusting and the relationship to cervical flexion: A retrospective case series of twenty-four patients. Asia-Pac Chiropr J. 2020;1.2:online only. https://apcj.rocketsparkau.com/anterior-thoracic-adjustment--getzoff
- Getzoff H. A primary cranial analysis and adjustment method for all three Sacro Occipital Technique (SOT) Categories: A retrospective study of 85 patients. Asia-Pac Chiropr J. 2023;4.2. apcj.net/Papers-Issue-4-2/#GetzoffCranial
- Getzoff H. Sacro Occipital Technique (SOT): A Systems Driven Method of Chiropractic. Asia-Pac Chiropr J. 2024;4.4. apcj.net/Papers-Issue-4-4/#GetzoffSOTSystem
- Getzoff H. Sacro Occipital Technique (SOT): Category Two: Systems integration. Asia-Pac Chiropr J. 2024;5.1. apcj.net/Papers-Issue-5-1/#GetzoffSOTCat2
- Getzoff H. Sacro Occipital Technique (SOT): Documentation and recording system. Asia-Pac Chiropr J. 2024;5.2. apcj.net/Papers-Issue-5-2/#GetzoffSOTDocumentation
- Getzoff H. The Atlas Vertebrae and its role in the function of the Sacro Occipital Technique (SOT) Categories. Asia-Pac Chiropr J. 2025;5.4. apcj.net/Papers-Issue-5-4/#GetzoffAtlasinSOT
- Getzoff H. Chiropractic Manipulative Reflex Technique: Based on the work of Major Bertrand DeJarnette, DO, DC [Book Review]. Asia-Pac Chiropr J. 2025;5.4. www.apcj.net/Papers-Issue-5-4/#GetzoffReviewCMRT
- Getzoff H. Sacro Occipital Technique (SOT): Questions and Answers (Q+A). Asia-Pac Chiropr J. 2025;6.1. www.apcj.net/Papers-Issue-6-1/#GetzoffSOTQandA
Hyperemesis Gravidarum helped with Vitamin K and Vitamin C: A Case Report
This case report is important as it is one of the few cases recorded that uses a novel approach to resolving HG as quickly as possible. It is also unusual in that it references older research observations that showed promising results with relative safety.
Resolution of Adhesive Capsulitis following Chiropractic care and Applied Kinesiology (AK): A case report
With regard to the efficacy of Chiropractic adjustments specifically for shoulder complaints, the current evidence is limited, consisting of one small pilot study, a qualitative study, and a number of case reports, of which this is one.

Improvement in Speech, Primitive Reflex Integration and Neurodevelopmental Dysregulation in a two-year-old male under Chiropractic care: A Chiropractic paediatric case report
Notably, the patient’s speech developed quickly, with the patient going from learning 1-2 new words per day to learning up to twenty new words per day. The mother described this as an ‘explosion’ in his speech. After twelve weeks, the patient remarked ’I’m so happy I can talk now’. His mother described being ‘blown away’ by the changes.
AU Lead: Jenna Godfrey, BSc, MClinChiro, ACCP. Private practice of Chiropractic, Newcastle Australia. e: hello@childrenschiropractic.com.au
AU 2: Ruth Postlethwaite, BBiomedSc. Writer, ASRF.
Background: A two year old male was presented for Chiropractic care by his mother with chief complaints of delayed speech, generalised low postural tone, persistent primitive reflexes, emotional dysregulation, and general fussiness.
Intervention: The patient received a short course of Chiropractic care, with all interventions modified to be age appropriate. This included diversified, drop-piece, and activator-assisted spinal and pelvic adjustments, cranial releasing techniques, soft tissue work, and a prescribed home exercise programme targeting left-body stimulation, proprioceptive joint distraction, and gross motor activation.
Outcomes: The patient’s mother noted fast and notable improvements in social engagement, speech, imaginative play, emotional regulation and gross motor competence, alongside the chiropractors observation of improvements in objective findings. The patients health index also rose from 58/100 to 82/100 (within the target range) over the course of care.
Conclusion: This case demonstrates an association between subluxation-based Chiropractic care and rapid improvement in speech, neurodevelopment, and emotional regulation in a two-year-old male with persistent primitive reflexes. This is consistent with the core Chiropractic paradigm, wherein subluxation may impact developmental maturation, and that Chiropractic care may facilitate improved nervous system function.
Indexing Terms: Chiropractic; Subluxation; paediatrics; delayed speech; primitive reflexes; emotional dysregulation.
Cite: Godfrey J, Postlethwaite R, McIvor C. Improvement in Speech, Primitive Reflex Integration and Neurodevelopmental Dysregulation in a two-year-old male under Chiropractic care: A Chiropractic paediatric case report. Asia-Pac Chiropr J. 2026;7.1. https://www.apcj.site/GodfreySpeech.pdf
Introduction
In the last decade Chiropractic researchers have made significant leaps in the evidence for the neurological impacts of Chiropractic, and the prevalence of neurodevelopmental disorders in children has increased by 40%.
We now have research indicating that Chiropractic care increases neural plasticity and sensorimotor integration. (Haavik and Murphy, 2007; Haavik and Niazi, 2024) While these studies were undertaken using adult populations, there is an increasing amount of case report data detailing individual cases of paediatric patients showing indications of neurodevelopmental improvement, including integration of retained primitive reflexes, concomitant with Chiropractic care. (Doyle, 2021; Fairest and Russell, 2019; Steinberg and Postlethwaite, 2022)
Additionally, a retrospective study of 37 paediatric patients with neurodeflective (also known as neurodevelopmental) disorders showed significant improvements in autonomic nervous system balance following subluxation based care. (Holt and Spoelstra, 2022) The study, which used clinical and educational tools to assess progress, revealed significant improvements in processing, engagement, learning and connection to surroundings across the cohort.
But perhaps most notably, statistics emerging in 2022 have revealed that in the decade prior, diagnoses of autism and other neurodevelopmental disabilities increased by 40%. (Shaw and Williams, 2022) This represents a significant challenge for parents and health professionals alike. Moreover, it is a challenge for Chiropractors and Chiropractic researchers to enter the conversation when it comes to bringing these two worlds together and presenting Chiropractic as a potentially vital part of infant and paediatric neurodevelopment.
Language
Within this picture, speech and language delay is among the most prevalent developmental concerns in early childhood. Current estimates show that prior to Covid-19, speech delay in preschool children sat at an average of 9%. Bartlett and Franklin (2023) found that children who turned two between September 2000 and March 2023 were more likely to be diagnosed with speech delay, which now sat at an average prevalence of 16.9%.
Delays in expressive and receptive language acquisition carry consequences that extend well beyond communication, with longitudinal research linking early speech delay to later difficulties in literacy, academic achievement, social competence, and mental health. (Johnson et al, 2010) While speech-language pathology remains the primary intervention pathway for these children, a growing body of clinical literature suggests that speech and language development is not an isolated function but rather one that emerges from, and depends upon, the broader maturation of the nervous system. For a subgroup of children, the persistence of early neuromotor patterns, specifically, the retention of primitive reflexes, may represent an under-appreciated contributor to developmental delay across multiple domains, including language.
Primitive reflexes
Primitive reflexes are involuntary, stereotyped movement responses mediated at the level of the brainstem and spinal cord. They emerge during foetal development and are present at birth as essential survival mechanisms, governing the infant’s ability to feed, breathe, orient toward stimulation, and respond to threat. (Modrell and Tadi, 2023) Under typical developmental conditions, these reflexes are progressively inhibited and integrated within the first twelve months of life as higher cortical structures mature and assume functional dominance. This process of integration is not merely the suppression of reflex activity; it is understood to represent the active development of cortical inhibitory circuits that underpin voluntary movement, postural stability, sensory processing, and cognitive function. When this integration fails to proceed normally, whether due to birth trauma, intrauterine stress, illness, or suboptimal neurological development, the reflexes persist beyond the expected window, a phenomenon referred to as retained or aberrant primitive reflexes.
Retained primitive reflexes have been associated with a wide spectrum of developmental, postural, and behavioural difficulties. Persistently active reflexes create competing neurological demands that interfere with voluntary motor control, balance, and coordination, as the nervous system must simultaneously manage both reflex-driven and intentional movement. (Goddard-Blythe, 2022) Clinically, retained reflexes have been linked to poor postural tone, vestibular dysfunction, difficulties with fine and gross motor skills, sensory hypersensitivity, poor impulse control, emotional dysregulation, and attention difficulties. The ongoing neurological 'noise' generated by unintegrated reflexes is thought to place increased demands on the central nervous system, reducing the available cognitive and regulatory resources for higher-order tasks, including language acquisition, social learning, and emotional self-regulation. (Martello, 2023)
Furthermore, the neurological burden imposed by retained reflexes broadly, through its impact on sensory integration, attention, and arousal regulation, may indirectly compromise the child’s capacity to engage with and benefit from language-rich environments. The speech pathologist’s observation that a child with delayed language also presents with postural markers of reflex retention is therefore clinically significant, and represents an important intersection between disciplines.
Subluxation-based care
How subluxations and subluxation-based care may impact the neurological systems that feed into reflex integration, neurodevelopment, speech delay and other issues remains largely theoretical, though larger scale clinical evidence is emerging. For parents, it is important to note that subluxation is not limited to the adult population. In the paediatric context, subluxations may arise from the mechanical forces of labour and delivery, including the use of obstetric interventions such as cervical ripening agents, artificial rupture of membranes, or instrumental delivery, as well as from the postural demands of early development and the cumulative strain of falls and motor learning.
The Chiropractic adjustment is proposed to restore normal segmental motion and afferent input, thereby supporting improved central nervous system processing. In the developing infant and toddler, this has implications not only for immediate physical function but for the neuroplastic processes underlying maturation, learning, and reflex integration.
This case report describes the presentation, assessment, management, and outcomes of a two-year-old male referred for Chiropractic care by a speech pathologist following a limited response to speech therapy. The case is noteworthy in that it illustrates the role of Chiropractic care in supporting neurodevelopmental outcomes in a paediatric patient, and highlights the interdisciplinary collaboration in the assessment and management of developmental delay.
Case details
A two-year-old male was presented for Chiropractic care at a paediatric-specific clinic on referral from a speech pathologist. At the time of presentation, the family was self-managing his speech development, and was not under the care of any other health professional. The primary concerns prompting his engagement with the speech pathologist and then the Chiropractor were delayed speech, low tone, general fussiness and unsettled moods, low resilience and general dysregulation.
The mother reported having an unremarkable pregnancy, which she termed ‘good’ while also noting significant occupational stress throughout the gestational period. Labour was induced using Cervadil tape, with a manual rupture of membranes performed the following day.
The patient was born at 40 weeks and six days gestation, arriving rapidly approximately ten minutes after rupture of membranes. Both mother and infant recovered well in the immediate postpartum period. Developmental milestones were described as largely on track, with the patient sleeping well, feeding well, and meeting gross motor benchmarks. However, the mother noted that he had always been characteristically ‘whingey’ and always wanted to be held, suggesting a baseline pattern of heightened regulatory demand from early infancy.
Prior to Chiropractic presentation, the patient had completed five to six sessions with a speech pathologist. During this time, some gradual progress in speech was observed; however, the speech pathologist identified postural and movement patterns that raised the possibility of retained primitive reflexes contributing to the patient’s developmental difficulties. On the basis of this clinical observation, the family was directed to seek assessment at the Australian Children's Chiropractic Centre, where a comprehensive neurodevelopmental Chiropractic assessment was undertaken.
Clinical findings
Upon presentation at the clinic a thorough history and examination was taken, during which a standardised paediatric Chiropractic protocol was used to assess cranial bone function, cervical and spinal range of motion, cranial nerve function, peripheral joint mobility, muscle strength and activation, neurological reflexes, primitive reflex testing, postural reflexes and tone assessment as well as gait analysis and postural photography.
Cranial bone function assessment identified restrictions at the left coronal suture, the squamous suture, the left parietal bone, and the right temporal bone. Cervical range of motion was restricted in flexion, left lateral flexion, and right rotation to a mild-to-moderate degree. Mid-thoracic range of motion was limited in extension and left lateral flexion, and the lumbar spine demonstrated restricted left lateral flexion. A pelvic extension restriction was also identified.
Peripheral assessment noted reduced mobility at the left ankle. Cranial nerve testing revealed poor bilateral pupil constriction. Vertebral subluxations were identified at the left anterosuperior occiput, C1, T3–5, L4, and S2.
Muscle strength and activation testing demonstrated decreased postural tone in both flexion and extension. Deep tendon reflexes were diminished bilaterally at the patella and Achilles tendons, and on the right side at the biceps. These findings were consistent with an overall pattern of reduced neurological tone and diminished efferent output through the lower motor neuron pathways.
Primitive reflex testing revealed persistent expression of the rooting reflex, palmar grasp, tonic labyrinthine reflex (TLR), asymmetrical tonic neck reflex (ATNR; moderate on the left, mild on the right), Perez reflex, right Galant reflex, and plantar grasp. The symmetrical tonic neck reflex (STNR) was also persistently present on postural reflex assessment. The retention of these reflexes beyond the expected developmental window represented a central feature of the clinical picture, with implications for postural control, motor coordination, and neurological integration.
Gait assessment revealed a shortened right leg stance phase with associated hip rotation, and reduced right-sided shoulder abduction during the swing phase. Posture assessment, conducted using a combination of photographs and gait video footage given the patient's age and compliance limitations, identified a left shoulder elevation and left head tilt. These postural asymmetries were considered consistent with the subluxation pattern identified and the persistent primitive reflex profile.
Management
Following assessment the patient was placed on a Chiropractic care plan with the immediate goal to support optimal nervous system function by addressing identified subluxations, thereby facilitating improved neurological firing, maturation, and integration. The long-term aims were to support progress in central postural tone, primitive reflex integration to age-appropriate levels, and improved gross motor function, gait, and balance. This was all in service of helping support this patient to function at his best, ultimately building a stronger brain and body connection, and support physical and neurological function.
The care plan was structured across three phases:
- an initial intensive phase of twice-weekly appointments for six weeks (inclusive of a formal clinical review and written review report in the final week)
- a consolidation phase of once-weekly visits for a further six weeks; and
- a maintenance phase of fortnightly appointments for six visits, again concluding with a clinical review and written report.
Chiropractic care was delivered using a multi-modal approach tailored to the patient’s age, presentation, and tolerance. This included age-appropriate diversified manual adjusting, drop-piece technique, and activator-assisted adjustments to the identified subluxation levels. Cranial releasing techniques were applied to address the identified cranial bone restrictions. Soft tissue therapy was incorporated as clinically indicated. All techniques were applied with forces appropriate for a two-year-old paediatric patient.
A home exercise programme was prescribed to complement in-clinic care. This focused on three key areas: left-body stimulation to address the observed lateralised reflexes and asymmetrical findings; proprioceptive joint distraction activities to support sensory integration and body awareness; and ‘big brain stimulation’ through gross motor play and large movement activities designed to support primitive reflex integration and cortical development.
Outcomes
While the patient was checked prior to adjustments at every visit, formal clinical reassessments were conducted at defined intervals throughout the care plan using the same battery of measures applied at initial presentation. The clinic’s health index, which aggregates findings across the assessment domains into a composite score out of 100, was used as a standardised tracking tool. At the initial presentation, the patient’s health index score was 58. By the first formal review, this had improved to 78, and by the third review, the score had reached 82 which exceeded the target threshold of 80.
Significant improvements in primitive reflex integration, body awareness and control and postural tone were all noted, along with significantly decreased subluxation patterns. Postural strength and reflexes were now normal. All primitive reflexes had integrated with the exception of the Asymmetrical Tonic Neck Reflex. All muscle testing was now within appropriate limits. Cranial nerve testing was also returning to normal, symmetrical results. However, some light sensitivity remained, and left coronial suture restriction remained. Subluxation patterns had now significantly reduced, with improvements noted at the Right Anterosuperior occiput, T3, L4 and S1.
Notably, the patient’s speech developed quickly, with the patient going from learning 1-2 new words per day to learning up to twenty new words per day. The mother described this as an ‘explosion’ in his speech. After twelve weeks, the patient remarked ’I’m so happy I can talk now’. His mother described being ‘blown away’ by the changes.
Alongside this, the parent observed substantial improvements in social engagement, including the development of peer friendships at daycare and in community settings, as well as meaningful development in imaginative play and improved gross motor skills including independent balance bike riding. Emotional regulation also improved markedly, with the patient demonstrating a greater capacity to identify and communicate his emotional state. He appeared to be generally more comfortable in his body, and better regulated in terms of mood, tone and in general.
Discussion
Chiropractic care for a child is also care for the whole household. In this case, the patient is able to communicate now which has relieved a lot of daily frustrations and emotional outbursts impacting not only him but his family. He has an overall happier life at daycare and home. He has better control over his body physically. Primitive reflexes have integrated which can help the patient to feel safer in his body and show less dysfunction. This can also help at school and with further learning and development.
Notably in this case, Chiropractic care was the only change to the patient’s life at the time and therefore it’s likely to have contributed by supporting neurodevelopment and co-regulation through subluxation-based care and recommended exercises.
This case demonstrates a clinically meaningful pattern of improvement in speech, neurodevelopment, postural tone, and emotional regulation following subluxation-based chiropractic care in a two-year-old male with persistent primitive reflexes and developmental delay. The trajectory of change, particularly the rapid acceleration in expressive language within the first weeks of care, is consistent with the hypothesis that resolution of neurological dysfunction may facilitate developmental processes that have been impeded by spinal and cranial subluxation.
The central theoretical framework underpinning this case is the relationship between vertebral subluxation, neurological function, and neurodevelopmental maturation. It is proposed that segmental dysfunction along the spine and cranium may create afferent interference that disrupts the normal maturation and integration of primitive reflex pathways.
The patient’s response to care also highlights the potential value of interprofessional collaboration in the management of paediatric developmental delay. In this case, the referral from a speech pathologist who observed postural indicators of retained reflexes during the course of her own treatment plan was the direct pathway to chiropractic assessment. This interdisciplinary awareness enabled an expanded approach to the patient's care that the speech pathology intervention alone had not fully achieved.
Chiropractic care was the only change introduced to the patient’s management at the time these improvements were observed, which supports its role as the most plausible contributing factor. However, it is important to acknowledge that this case represents a single patient, and that natural developmental maturation and the carry-over benefit of prior speech therapy cannot be entirely excluded as contributing influences.
Despite these limitations, the case adds to a growing body of literature suggesting that chiropractic care may play a meaningful role in supporting neurodevelopmental outcomes in paediatric patients with persistent primitive reflexes, low postural tone, and associated developmental and regulatory difficulties. The findings suggest that a Chiropractor’s assessment of cranial, spinal, and neurological function may offer a complementary perspective in the multidisciplinary evaluation of children with developmental delay.
Conclusion
This case report documents significant improvements in expressive language, primitive reflex integration, postural tone, emotional regulation, and overall developmental function in a two-year-old male following a course of subluxation-based chiropractic care.
The outcomes observed across serial clinical reassessments and parent reports suggest that addressing spinal and cranial subluxation may facilitate neurological maturation in paediatric patients with persistent primitive reflexes and associated developmental concerns.
Given the limitations inherent in single-case reporting, prospective cohort studies and randomised controlled designs are warranted to further investigate the efficacy of chiropractic care in this population.
Bibliography
- Bartelt K, Gracianette M, Deckert J, et al Childhood Speech Development Delays Increasing Since the Start of the Pandemic. Epic Research. https://epicresearch.org/articles/childhood-speech-development-delays-increasing-since-the-start-of-the-pandemic. Accessed on May 29, 202
- Doyle M. (2021). Improvements in developmental delay in a female child following chiropractic care: a case report and selective review of the literature. Journal of Clinical Chiropractic Pediatrics. Vol. 20. Iss 2. https://jccponline.com/doyle20-02.pdf
- Fairest C, Russell D. (2019), “Improvement in behavior and attention in a 7-year-old girl with ADHD receiving chiropractic care: a case report and review of the literature,” Journal Clinical Chiropractic Pediatrics, Volume 18, No 1. http://jccponline.com/ADHD.pdf
- Goddard Blythe S, Duncombe R, Preedy P. et al. (2022). Neuromotor readiness for school: the primitive reflex status of young children at the start and end of their first year at school in the United Kingdom. Education 3-13, 50(5), 654–67. https://doi.org/10.1080/03004279.2021.1895276
- Haavik-Taylor H, Murphy B. Cervical spine manipulation alters sensorimotor integration: A somatosensory evoked potential study.Clin Neurophysiol. 2007;118(2):391-402. DOI 10.1016/j.clinph.2006.09.014
- Haavik H, Niazi IK, Amjad I, et al. Neuroplastic Responses to Chiropractic Care: Broad Impacts on Pain, Mood, Sleep, and Quality of Life. Brain Sci. 2024, 14, 1124.
- Hock S, Spoelstra A. Improved Brain Development in 37 Children Undergoing Chiropractic Care for Correction of Vertebral Subluxation: A Retrospective Analysis of Health Outcomes. J. Pediatric, Maternal & Family Health. 2022;86-94.
- Johnson CJ, Beitchman JH, Brownlie EB. (2010). Twenty-year follow-up of children with and without speech-language impairments: Family, educational, occupational, and quality of life outcomes. American Journal of Speech-Language Pathology, 19(1), 51–65. https://doi.org/10.1044/1058-0360(2009/08-0083)
- Law J, Boyle J, Harris F, et al. (2000). Prevalence and natural history of primary speech and language delay: findings from a systematic review of the literature. Int J Lang Commun Disord. Apr-Jun;35(2):165-88. DOI 10.1080/136828200247133.
- Martello J. (2023). Persistent Primitive Reflex and Developmental Delay in the School-Aged Child. The Journal For Nurse Practitioners. Vol. 19. Iss. 10. November 2023 DOI https://doi.org/10.1016/j.nurpra.2023.104767
- Modrell AK, Tadi P. Primitive Reflexes. [Updated 2023 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554606/
- Shaw KA, Williams S, Patrick ME, et al. Prevalence and Early Identification of Autism Spectrum Disorder Among Children Aged 4 and 8 Years — Autism and Developmental Disabilities Monitoring Network, 16 Sites, United States, 2022. MMWR Surveill Summ 2025;74(No. SS-2):1–22. DOI: http://dx.doi.org/10.15585/mmwr.ss7402a1
- Steinberg B, Postlethwaite R, McIvor C. Improvement in Physical Resilience and Management of ADHD in a 12-year-old Male under Chiropractic Care: A case report. Asia-Pac Chiropr J. 2022;2.6. apcj.net/papers-issue-2-6/#SteinbergResilience
About the Case Report project
This Case Report is a part of the ASRF Case Report Project, a project designed to gather client studies from chiropractors and transform them into much-needed case reports, focused on the effects of chiropractic care on clinical presentations highly relevant to chiropractic, such as stress, immunity and adaptability.
This valuable project is made possible by the generous fundraising and contributions of ASRF supporters.
A novel approach to Neurorehabilitation for persisting Post Concussion Syndrome with occupational reintegration in 2 males aged 34 & 43: A Case Series of 2
Persisting post-concussive symptoms (PPCS), defined as three or more symptoms persisting beyond three months after mild traumatic brain injury, affect 24-43% of concussed individuals and cause substantial occupational disability.
This case series of two working-age men with PPCS >12 months documents multimodal neurorehabilitation and objective recovery metrics alongside return-to-work outcomes. [Ed note: one of the occupational outcomes will surprise you]
AU: David Richardson, BAppSc(Chiropr). Chiropractor, Eden NSW. e: david@edenchiropractic.com.au
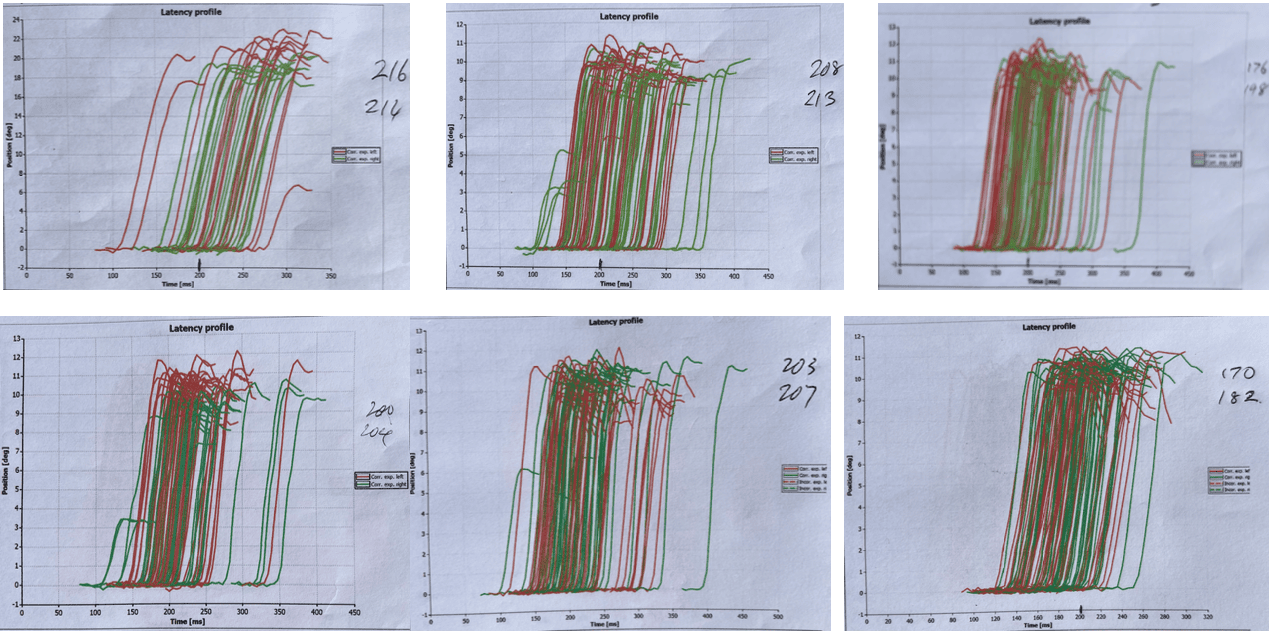
Of note in this series is that from the top left, the initial plot shows a sparsity of readings, indicating that the brain initiated eye movements that were too slow to be recorded while the spread of the entire group represents the brain’s inability to reproduce an identical saccade to the same target with the same timing consistently. Clearly a sign of a dysfunctional nervous system.
The top middle plot shows some green rightward looking preemptive saccades to the left of the main group, which are erroneously initiated by the superior colliculus of the brain stem. Again a dysfunctional reaction to a voluntary saccade. Throughout the treatment period there is a positive progression, however the disparity between sides represents a neurological conflict.
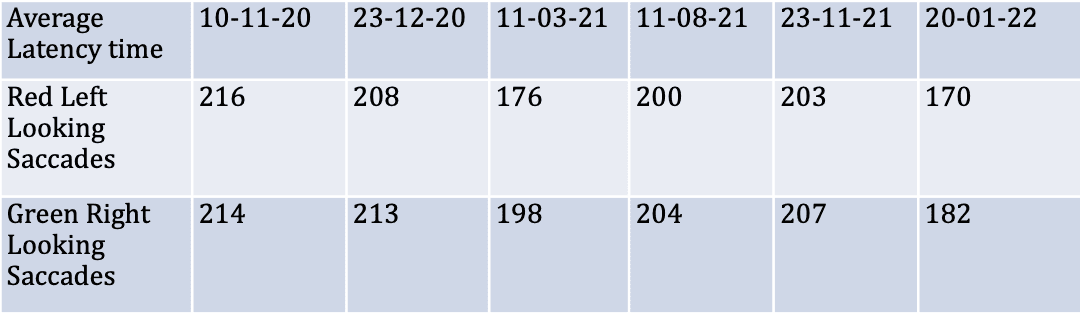
Force Plate Posturography
Pre-treatment instrumented force plate posturography demonstrated impaired postural stability consistent with the persistent neuromotor control deficits documented in chronic PPCS. Force plate measures have been shown to detect ongoing functional impairment in PPCS populations (12) and to identify deficits not apparent on conventional clinical balance tests such as the Balance Error Scoring System. (11) Athletes and workers with mTBI history demonstrate significantly poorer stability than controls during balance perturbations and quiet stance, with differences accentuated in eyes-closed conditions, (11) a pattern consistent with the reliance on visual substitution for vestibular impairment observed clinically in PPCS. Pre- and post-treatment posturographic data are presented in Figure 2
Force Plate Analysis: Pre vs Post Treatment
Pre-treatment
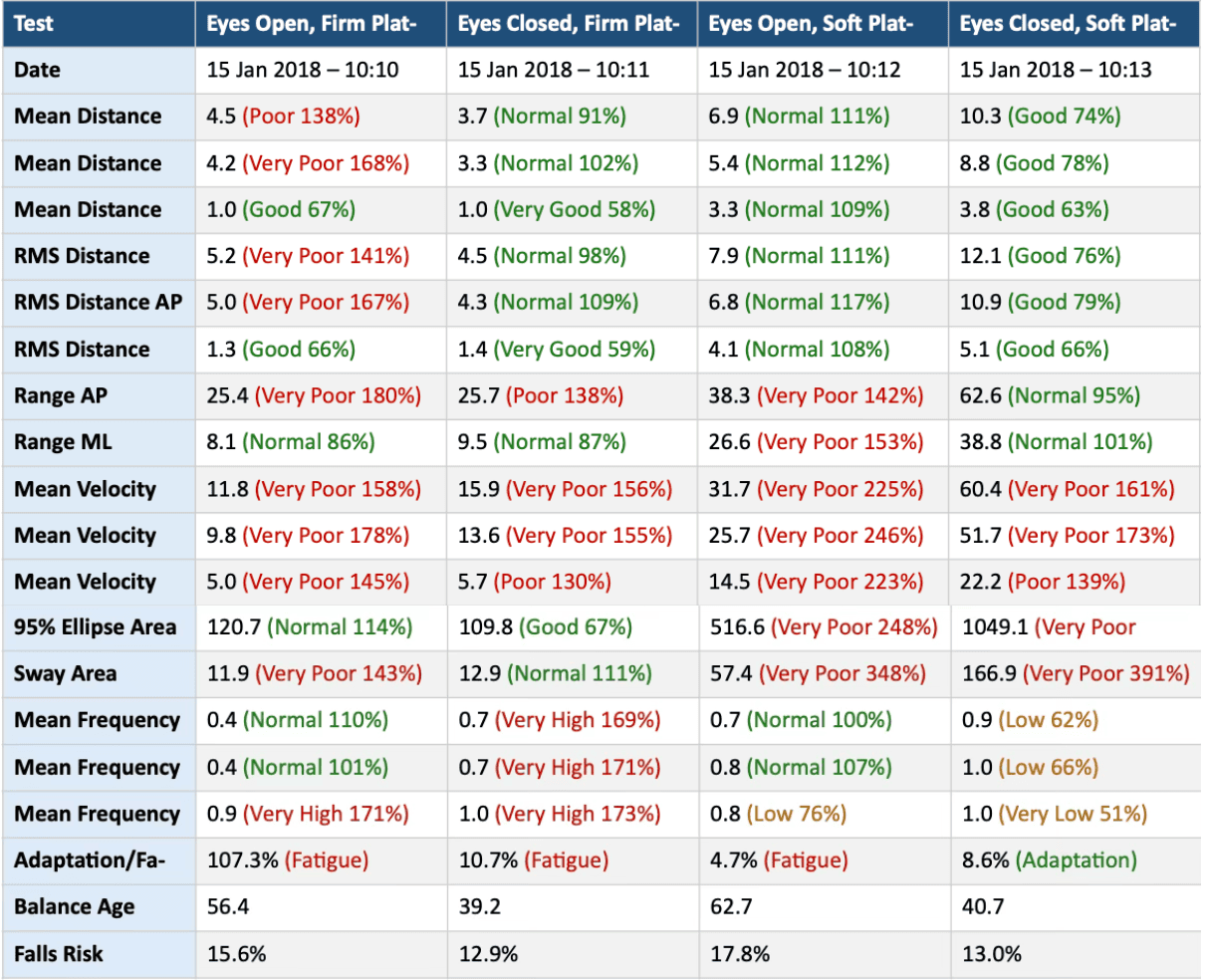
Post treatment
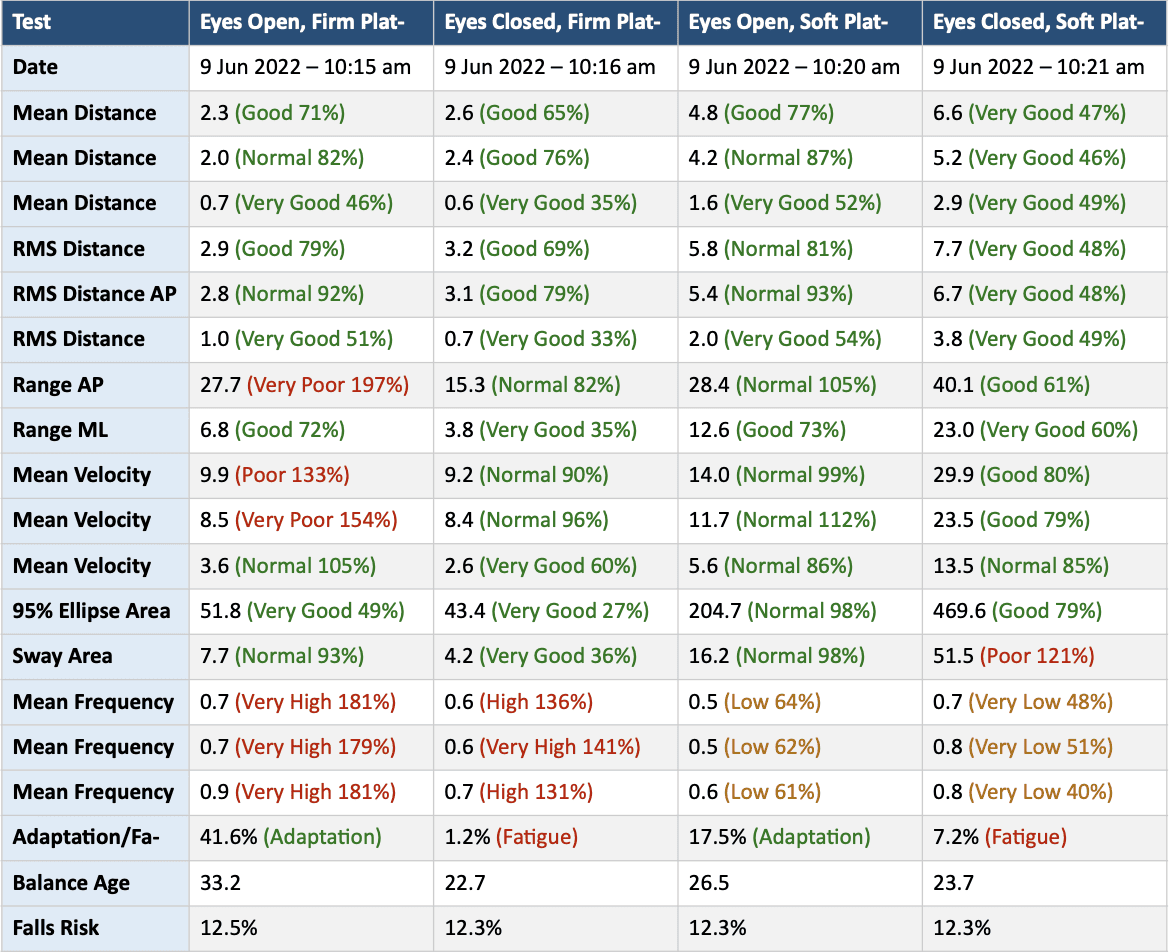
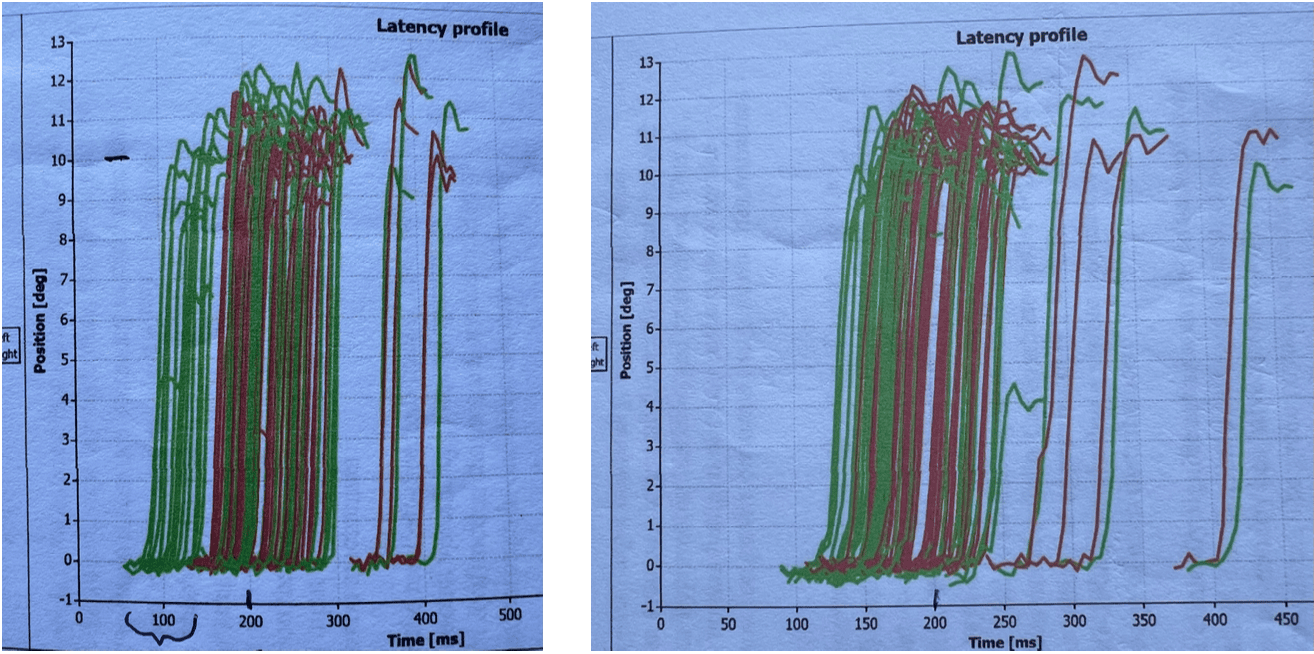

Force Plate Posturography
Pre-treatment force plate posturography confirmed objective postural instability consistent with persistent balance impairment in chronic PPCS. (11, 12) Post-treatment force plate posturography demonstrated objective improvement from baseline.
This force plate analysis represents severe multi system postural control failure, characterised by critical visual dependency with near total postural collapse without vision on a firm surface. It indicates that proprioception alone on a firm surface is completely inadequate to maintain upright stability. He is entirely dependent on visual input for posture control on a firm surface. When vision is removed the postural control system fails rather than successfully switching to proprioceptive and/or vestibular references, as would normally occur. Recall that this chap, on initial presentation, had to lean against a wall in order to talk!
The paradoxical relative preservation of performance on a soft platform compared to a firm platform without vision indicates that the patient cannot effectively use firm surface proprioceptive input as a postural reference when visual input is unavailable. This suggests disruption of the central integration of proprioceptive and vestibular signals, likely at the level of the vestibular nuclei and their cerebella connections, which are responsible for weighting and combining these inputs for postural control.
The absence of within-trial adaption in each of the 4 testing conditions confirms that this patient has no postural adaptive reserve, every condition taxes the system to its absolute limit.
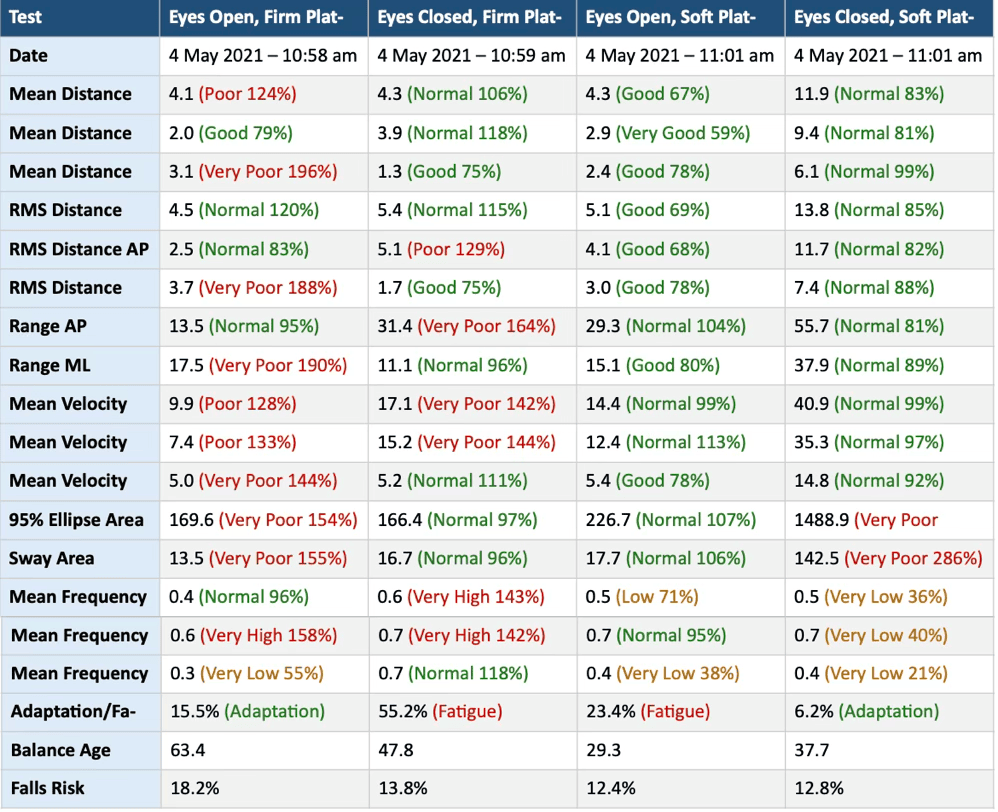
Diagnostic Assessment
Overview of Assessment Battery
Both patients underwent comprehensive assessment structured across the objective domains: autonomic, saccadic, postural stability, cervical, neurological and physical examination with oculomotor assessment for convergence insufficiency (P2 only). The assessment battery reflects the multi-domain presentation of PPCS, encompassing vestibular, oculomotor, cognitive, autonomic, cervicogenic, and postural systems, (5, 7) and the recognised need for objective rather than purely symptom-based diagnostic approaches to this population given the absence of a consensus diagnostic standard. (21)
Saccadometry
Saccadometry was performed in darkened conditions, consistent with published protocols. (9) The overlap (OVL) paradigm was assessed. Parameters recorded included bilateral latency (ms), amplitude (degrees), peak velocity (deg/s), and main sequence ratio (Q value) at each session. Latency distribution profiles and phase plots were generated for each paradigm to characterise trajectory variability.
Pre-treatment saccadometry for P1 demonstrated elevated latency with bilateral asymmetry and high inter-trial trajectory variability, consistent with frontal-cerebellar circuit disruption. The latency was elevated relative to published normative data8 with wide latency scatter consistent with poor control of saccade initiation, a pattern that has been shown to correlate with corpus callosum white matter diffusivity, reduced executive function performance, and PPCS symptom burden. (9)
Post-treatment saccadometry demonstrated improvement from baseline. Pre-treatment saccadometry for P2 demonstrated elevated latency, reduced peak velocity, and disordered trajectory profiles consistent with the oculomotor circuit disruption characteristic of chronic PPCS.8,10 Post-treatment saccadometry demonstrated objective improvement.
Force Plate Posturography
Instrumented force plate posturography was used to quantify postural stability through measurement of centre-of-pressure displacement during standardised standing tasks. Force plate-based posturography has been shown to detect ongoing neuromotor control impairment in PPCS populations (12) and to identify deficits not apparent on clinical balance tests alone, with instrumented measures sensitive to postural abnormalities persisting well beyond symptomatic resolution in both acute and chronic mTBI. (11)
Pre-treatment posturography for both P1 and P2 demonstrated impaired postural stability. Post-treatment posturography demonstrated objective improvement from baseline in both patients.
Oculomotor Assessment
Both patients underwent assessment of Near Point Convergence (NPC). Convergence insufficiency was diagnosed on the basis of a receded NPC, consistent with the diagnostic criteria used in published PPCS convergence insufficiency studies. (18) The prevalence of symptomatic convergence insufficiency in adults with PPCS has been reported at 20.4%18 and at 23-42% in military populations, (19) placing the finding within an expected range for this diagnostic context.
Physical and Neurological Examination
Both patients underwent physical examination including cervical range of motion assessment, segmental motion palpation, upper and lower limb neurological examination, and cranial nerve screening.
Both patients demonstrated cervical segmental restriction and dysfunction consistent with cervicogenic contribution to headache and dizziness. Neurological examination was otherwise consistent with multi-domain PPCS without focal lateralising deficit.
Diagnostic Challenges
Several diagnostic challenges were present in both cases. There is currently no global consensus on the objective measures that establish a definitive diagnosis of PPCS in any age group, (21) and the diagnosis remains clinical rather than biomarker-confirmed. The objective assessment tools used in this series, quantitative saccadometry, and force plate posturography, are not universally available in primary or secondary care settings, creating inequity in access to this level of diagnostic evaluation for PPCS patients.
Second, both patients presented beyond twelve months post-injury, at which point the neurological deficit profile reflects the compound effects of the initial injury, maladaptive neuroplasticity during the intervening period, physical deconditioning, and possible learned postural and behavioural compensatory strategies. Disentangling these contributions from the primary injury deficit was not possible from assessment data alone and was not required for treatment planning.
Third, neuro-imaging was not performed at the time of assessment. Both patients had presented beyond the acute phase at which structural neuro-imaging was performed, clinical assessment did not reveal red flags warranting urgent imaging. The absence of neuro-imaging is a recognised limitation of clinical case series in this population and precludes characterisation of any structural correlates of the objective neurophysiological findings.
Diagnosis
Both patients were diagnosed with persisting post-concussive syndrome (PPCS) on the basis of a documented history of mTBI, symptom duration exceeding three months, and the presence of three or more persistent post-concussive symptoms across multiple domains at the time of presentation. The diagnosis is consistent with the 2023 American Congress of Rehabilitation Medicine diagnostic criteria for concussion and mTBI, (21) which define mTBI as a traumatically induced physiological disruption of brain function with Glasgow Coma Score 13-15, loss of consciousness under 30 minutes where present, and post-traumatic amnesia under 24 hours.
The multi-domain objective abnormalities documented across the assessment battery, saccadometric frontal-cerebellar disruption (both), postural instability (both), and convergence insufficiency (both), were interpreted as consistent with the distributed neurophysiological consequences of chronic mTBI affecting brainstem, cerebellar, oculomotor, and autonomic pathways, and as representing the objective substrate of the presenting symptom profile.
Alternative diagnoses considered and excluded included: primary vestibular disorder (no unilateral peripheral pattern on examination, no BPPV features, no Menière’s disease features); functional neurological disorder (objective findings on quantitative instrumented assessment inconsistent with a purely functional aetiology); primary mood disorder driving somatic amplification (possible contributory factor not formally excluded but not the primary diagnosis given the objective neurophysiological profile); and cervicogenic syndrome as the primary diagnosis (cervicogenic pathology was identified in both patients and managed as a contributing factor, but the distributed multi-domain objective findings were not consistent with cervicogenic aetiology as the sole explanation).
Prognosis
At the time of first assessment, the prognosis for each patient was guarded given the chronicity of their presentations, the multi-domain objective neurophysiological deficit profiles, and the documented difficulty of achieving recovery in PPCS beyond twelve months. (6, 7) The absence of a prior structured multimodal rehabilitation programme for either patient was noted as a prognostically relevant factor, as both had exhausted standard management without benefit prior to referral.
For P1, the prognosis for functional improvement was considered reasonable given the absence of neurological red flags, the absence of a prior structured rehabilitation attempt targeting the documented objective deficit profile, and the patient’s motivation to return to his trade. The saccadometric dysmetria was a significant finding but was interpreted as reflecting a potentially reversible adaptive state rather than irreversible structural damage, on the basis of the absence of a focal deficit.
For P2, the prognosis was also considered reasonable for functional improvement, though complicated by the orthostatic tachycardia, which required specific rehabilitation addressing the autonomic system, (19, 20) and the cervicogenic component requiring physical management. (15, 16)
Both patients were counselled that the rehabilitation program would be individualised, protracted, and progressively dosed, and that the primary target was functional recovery and occupational reintegration rather than normalisation of all objective neurophysiological parameters.
Therapeutic Intervention
Shared Intervention Principles
Both patients received an individualised, assessment-driven, multimodal neurorehabilitation program. Interventions were selected and dosed on the basis of each patient’s specific objective deficit profile as identified at baseline assessment, consistent with the approach described by Ross et al (10) in which neuroplasticity and sensory entrainment created by rigorous, diagnostic- and problem-focused, structured neurorehabilitation are proposed as the mechanisms of efficacy in chronic PPCS.
The principle of progressive loading, beginning at a level within the patient’s tolerance and advancing difficulty systematically with demonstrated capacity, was applied across all components. No adverse events were reported during either patient’s treatment course.
Patient 1: Clinic-Based interventions
Vestibular stimulation via Orbital multi-axis rotational chair. The Orbital device delivers controlled rotation in sagittal roll, yaw, and pitch planes, providing vestibular stimulation patterns not reproducible through any natural daily activity. Multi-axis rotational therapy in the PPCS population has been associated with significant reductions in symptom severity, enhanced balance improvement, and faster recovery trajectories when added to standard neurorehabilitation protocols.
Saccade and oculomotor training using a head-mounted weighted helmet with laser targeting computer-generated randomly selected LARP and RALP diagonal plane target panels. The weighted helmet increases the proprioceptive and motor demand of head movement, while the laser-to-target task requires active VOR engagement with immediate visual feedback on accuracy, a prerequisite for cerebellar VOR adaptation. (22, 23, 24, 25, 26)
Sensorimotor integration as backwards treadmill walking with weighted ankles (0.5 kg per ankle) and concurrent juggling for five minutes per session. This dual-task paradigm diverts attentional resources from conscious postural control, training automatic vestibular-postural responses while the visual system is engaged in the juggling task. The backwards direction specifically challenges the vestibular system by removing the predictive visual flow available during forward locomotion.
Lighted target panel tapping using random illuminated targets presented on a panel requiring rapid manual responses, beginning at slow presentation rates and progressively increasing in speed with demonstrated performance capacity. This trains upper limb reaction time, visuomotor processing speed, and hand-eye coordination.
Rhythmic entrainment therapy using audiovisual feedback signal synchronised with bilateral hand clapping on cue. Entrainment-based timing training, consistent in principle with the Interactive Metronome paradigm, has been shown in a randomised controlled pilot trial to significantly improve attention, immediate memory, and delayed memory in patients with persistent cognitive complaints following TBI when added to standard rehabilitation care, with effect sizes in the medium-to-large range. (27)
Spinal adjustments targeting identified cervical segmental dysfunction. Spinal manipulative therapy for cervicogenic headache has been supported by systematic review and meta-analysis with significant moderate-to-large short-term effects for headache frequency and intensity. (16)
Home program
One leg teeth balance exercise: a standing single-leg balance task while teeth cleaning to engage the trigemino-cerebellar proprioceptive pathway.
Diaphragmatic breathing in a five-second rhythm for one minute, three times per day, slow respiratory rate breathing to modulate autonomic tone and reduce sympathetic hyperactivation consistent with the post-concussive autonomic dysregulation. (28) This was documented with pupillometry (29, 30) to assist with patient compliance.
Vergence card: home vergence rehabilitation targeting the oculomotor convergence-divergence system.
iPad App saccade and pursuit training: horizontal anti-saccade training and diagonal pursuit exercises (up-right and down-left) for three minutes twice daily.
Breath-pause exercise: sudden full exhalation followed by maximal apnoea, progressively building toward one-minute sustained breath pause. This exercise modulates CO₂/O₂ balance and trains respiratory and autonomic regulation.
Head-turn walking: rapid side-to-side yaw head movements while walking, within symptom tolerance, providing a low-level continuous horizontal VOR stimulus during functional activity. (31)
Administration of therapeutic intervention
P1 completed 45 treatment sessions over 16 months. Clinic sessions were structured to deliver the full intervention battery with progressive task difficulty. The treatment table for P1 is presented in the Timeline section.
Changes in therapeutic intervention with rationale
Treatment intensity and task difficulty were progressively advanced throughout the 16-month course as P1 demonstrated improved performance capacity. The primary adaptive change across the treatment period was systematic progression of all tasks toward greater speed, complexity, and cognitive-motor demand, in line with the principle of progressive neurological loading. No abrupt changes in treatment type or direction were required. The 16-month duration reflects the protracted nature of recovery in chronic PPCS beyond twelve months post-injury and the extended timeline required to produce cumulative neuroplastic change in the context of the documented objective deficit profile.
Patient 2: Clinic-Based interventions
Vestibular stimulation via Orbital multi-axis rotational chair, as described for P1, with axis selection and dosing determined by P2’s specific vestibular deficit profile on assessment. Beginning with Yaw and progressing to Yaw with Roll, P2 progressively tolerated the stimulation without adverse effects.
Rhythmic entrainment therapy: bilateral hand clapping synchronised to a 54 Hz audiovisual beat. The 54 Hz frequency corresponds to the Interactive Metronome standard beat rate. Rhythmic entrainment therapy at this frequency trains sensorimotor synchronisation, neural timing, and frontal-cerebellar timing circuits implicated in cognitive processing speed, deficits consistently documented in PPCS. A randomised controlled pilot trial found that Interactive Metronome therapy added to standard rehabilitation care significantly improved attention, immediate memory, and delayed memory in soldiers with persistent cognitive complaints following blast-related TBI, with neuroplastic changes accounting for large proportions of the variance in neuropsychological outcomes. (27)
Sensorimotor Integration Reaction Timer panel training with the ‘gap scenario’. The gap paradigm presents a temporal gap (400ms) between target offset and the next stimulus, reducing fixation-related suppression of the superior colliculus and producing shorter saccadic latencies. This specifically targets the saccadic latency elevation documented on saccadometry, addressing the neural timing deficit at the subcortical level.
Head-mounted laser: tracing a wall map and navigating a maze at varying distances. This task requires sustained active head-eye coordination across spatial targets, engaging the VOR across the full range of head movement and demanding convergence and divergence across changing target distances, directly addressing P2’s convergence insufficiency in a functional movement context.
Diagonal saccade and pursuit exercises: saccades and smooth pursuits performed diagonally across a wall target at arm’s length. Diagonal plane exercises engage the LARP and RALP canal and oculomotor planes simultaneously, combining vestibular and vergence rehabilitation demands.
Repetitive Peripheral Somatosensory Evoked Potential (RPSEP) stimulation of the Trigeminal nerve (CN V) using a peripheral nerve stimulator applied at four locations along the Trigeminal distribution for one minute each. Trigeminal nerve stimulation produces somatosensory evoked potentials with cortical projections to the primary somatosensory cortex via brainstem relay, (32) and Trigeminal SEP provides an objective test of Trigeminal nerve function and its central connections through the brain-stem. (33) The Trigeminal nuclei in the pons are not anatomically contiguous with the vestibular nuclei but have direct functional interactions relevant to vestibular, autonomic, and oculomotor integration.
Repetitive stimulation at peripheral Trigeminal locations was applied to drive afferent brainstem input through these interconnected circuits as a component of the broader neurorehabilitation strategy.
Spinal adjustments targeting identified cervical segmental dysfunction, as described for P1.
Home program
Cervical stretching exercises: addressing identified range of motion restriction and muscle tension.
X2 VOR exercise performed slowly: active head movement while maintaining visual fixation on a moving target was performed at reduced speed consistent with P2’s tolerance, targeting gaze stabilisation through VOR adaptation.
One leg teeth balance exercise: as described for P1.
Isometric exercises five minutes daily to promote Myokine production while maintaining strength and joint loading without dynamic movement stress, appropriate for a patient with exercise intolerance in the early treatment phase.
Vergence card: home vergence rehabilitation for the convergence insufficiency directly identified on assessment.
Infinity Thumb exercise: looking firstly to the horizon then the tip of the outstretched thumb, followed by bringing the thumb to 6cm in front of the eyes and reversing, this trains convergence and divergence across the full range of binocular gaze, specifically addressing P2’s convergence deficit.
Deep knee bends (squats) 25 repetitions three times daily: lower limb strengthening and repeated postural loading providing an orthostatic and proprioceptive training stimulus.
Administration of therapeutic intervention
P2 completed 42 treatment sessions over 10 months. The treatment table for P2 is presented in the Timeline section.
Changes in therapeutic intervention with rationale
As P2’s convergence insufficiency improved with directed oculomotor rehabilitation, the visual demands of the laser map and maze exercise were progressively increased to maintain challenge at the convergence and divergence system. The reaction timer panel speed was systematically advanced with demonstrated improvement in response latency and accuracy. The vestibular rotation components were adjusted across sessions in response to P2’s tolerance and symptomatic response. The vocational reorientation that occurred during the latter portion of treatment, P2 undertaking online distillery manufacturing courses, was not a treatment modification but an adaptive patient-led functional outcome that emerged from improving capacity during treatment, and was supported as a purposeful and motivationally significant recovery milestone.
The 10-month treatment duration reflects P2’s rate of clinical progression within the constraints of his functional tolerance and the complexity of his multi-domain deficit profile.
Follow-up and outcomes
Patient 1
Clinician-assessed outcomes were documented through serial objective re-assessment across the treatment period. Progressive improvement was noted throughout the 16 months of treatment across all assessed domains.
Saccadometry: post-treatment data demonstrated improvement from baseline in latency, bilateral latency symmetry, and trajectory profile consistency in the overlap paradigm. Quantitative pre- and post-treatment saccadometric data are presented.
Force plate posturography: assessment demonstrated improved postural stability from the pre-treatment baseline. Pre- and post-treatment data are presented.
Patient-assessed outcome: at the completion of treatment, P1 reported feeling markedly recovered. This subjective assessment of recovery was consistent with the objective neurophysiological findings and directly preceded P1’s decision to seek re-employment in his trade. P1 subsequently returned to full-time employment as a qualified electrician. At the time of preparing this manuscript, P1 provided verbal confirmation that no exacerbations or recurrence of the initial signs or symptoms have occurred since resuming full-time work.
The post-treatment assessments described above constitute the follow-up diagnostic data for P1. No further formal follow-up assessment was scheduled beyond the treatment completion assessment. Ongoing monitoring was not conducted through additional neurophysiological testing at the time of manuscript preparation, as P1 reported full functional recovery.
P1 completed 45 sessions across a 16-month treatment period, indicating satisfactory adherence to the clinic-based program across an extended course. The sagittal roll component of the Orbital rotational chair, described as an atypical movement not reproducible in daily activity, was tolerated without vestibular exacerbation across the treatment period. Home program adherence was not formally measured by objective means; P1’s progressive improvement on all clinical and objective measures across sessions is consistent with adequate engagement with home exercise components between clinic visits. No tolerability concerns were documented during the treatment period.
No adverse events attributable to the treatment program were reported or documented for P1. No unanticipated events affected the treatment course. The absence of symptom exacerbation beyond the typical post-session fatigue expected in neurological rehabilitation is consistent with the progressive loading approach applied across all interventions.
Patient 2
Saccadometry: post-treatment assessment demonstrated improvement from the pre-treatment baseline across latency, peak velocity, and trajectory profile metrics in the overlap paradigms. Post-treatment data are presented in Figures 1 & 3.
Force plate posturography: post-treatment force plate assessment demonstrated improved postural stability from the pre-treatment baseline. Post-treatment data are presented in Figure 2.
Convergence: clinical convergence assessment at the completion of treatment demonstrated improvement in near point convergence (NPC=6cms) from the presenting deficit.
Patient-assessed outcome: P2 reported a remarkable improvement in his ability to progress through life across the 10-month treatment period. Towards the treatment completion P2 was feeling well enough to undertake online courses and to pursue vocational reorientation. He was not entirely pain-free at treatment completion and acknowledged the potential benefit of further treatment; however, he reported sufficient functional capacity to sustain his new vocational activities independently.
The unanticipated functional endpoint of P2’s rehabilitation, transition from spray painting to founding, operating, and staffing a distillery manufacturing business, was not the originally intended outcome of treatment but represents a remarkable and clinically meaningful vocational reintegration in a patient who entered treatment unable to resume his prior occupation and unable to engage in any employment or retraining.
The post-treatment assessments described above constitute the follow-up diagnostic data for P2. No further neurophysiological follow-up assessment was undertaken at the time of manuscript preparation. P2 remained engaged in his new vocational activities without scheduled clinical attendance, though he acknowledged the potential value of further treatment.
P2 completed 42 sessions across a 10-month treatment period, indicating satisfactory adherence across a protracted outpatient course. The vestibular rotation, RPSEP stimulation, sensorimotor integration components including spinal manipulation, were tolerated across the treatment period without documented intolerance. Home program adherence was not formally measured by objective means.
Progressive improvement of objective measures across sessions is consistent with sufficient engagement with home exercises to support the clinical gains documented. No significant tolerability concerns were documented during the treatment period.
No adverse events attributable to the treatment program were reported or documented for P2.
Discussion
Strengths
The primary strength of this case series is the use of serial objective neurophysiological assessment to document treatment response in parallel with the primary functional outcome of interest, occupational reintegration. The combination of quantitative saccadometry, and instrumented force plate posturography across the treatment period provides a multi-domain objective evidence base that is rarely reported alongside vocational outcomes in the PPCS literature.
Most published PPCS case series and retrospective studies rely on subjective symptom scales as primary outcome measures; the objective neurophysiological data presented here address a recognised gap in the evidence base. (5, 7)
Both patients represent a chronicity of presentation, PPCS exceeding twelve months, that is associated with poor prognosis in the broader literature and that is underrepresented in rehabilitation trial populations. (6, 7) The occupational outcomes are clinically meaningful beyond the neurophysiological data: P1’s full return to a safety-critical skilled trade and P2’s novel vocational self-employment represent outcomes that carry direct economic, psychological, and social significance for the patients and their communities.
A further strength is the explicit documentation of every intervention modality, its dosage, and its progression rationale, in compliance with CARE reporting standards, (34) which allows readers and future researchers to evaluate and potentially replicate the treatment approach.
Limitations
The absence of a control condition is the primary methodological limitation inherent to case series design. It is not possible to determine from two cases whether the observed improvements reflect the specific treatment program, the passage of time, regression to the mean, placebo response, or some combination of these. The CARE guidelines acknowledge this limitation as intrinsic to case report methodology (34) and the cases are presented as clinical observations rather than as evidence of treatment efficacy.
Neuro-imaging was not performed at either presentation. The absence of MRI data means that the structural correlates of the objective neurophysiological findings, including any white matter abnormalities consistent with diffuse axonal injury, or focal lesions that might explain the asymmetric components of the saccadometric data, cannot be characterised. This limits the mechanistic interpretation of the findings.
Formal standardised symptom questionnaires, such as the Rivermead Post Concussion Symptoms Questionnaire or the Post-Concussion Symptom Scale, were not administered. The absence of validated symptom severity scoring precludes direct comparison of symptom trajectories with published normative data and with outcomes reported in other PPCS rehabilitation studies using these instruments.
The contribution of individual treatment components to the overall outcome cannot be determined from the data available. Both patients received multimodal programs in which all interventions were delivered concurrently and progressively. The specific therapeutic mechanism responsible for the measured improvements cannot be isolated.
Home program adherence was not objectively monitored. The assumption that home exercises contributed to outcomes rests on clinical inference rather than documented compliance.
Finally, the asymmetry in available data across the two patients means that the full objective assessment battery is not directly comparable between cases.
Discussion of relevant literature
PPCS in working-age adults and occupational outcomes
Persisting post-concussive symptoms affect between 24% and 43% of those who sustain a concussion (5) and constitute a significant source of occupational disability. Silverberg et al. (35) demonstrated that even among mTBI patients who achieve a formal return to work, a substantial proportion experience ongoing productivity loss, with 60% reporting affected work productivity at six to eight months post-injury, and residual symptoms, depression, anxiety, and bodily pain continuing to impair work performance. This highlights that the boundary between ‘returned to work’ and ‘fully recovered occupationally’ is not clearly defined by RTW status alone, a distinction directly illustrated by the contrasting outcomes of P1 and P2 in the present series, where P1’s full return to a skilled and physically demanding trade represents a more complete occupational recovery than the term ‘RTW’ alone would convey.
Post-concussive symptom burden is the strongest predictor of failure to return to work at six months post-mTBI. (36) In a prospective cohort study (UPFRONT, n="1,151)," rates of complete return to work increased from 34% at two weeks to 77% at twelve months, but occupational factors influenced short-term RTW while symptom burden and psychological distress were the dominant predictors of long-term RTW.37 Both P1 and P2 in the present series presented with symptom burdens exceeding twelve months and failed to achieve RTW through prior standard management, placing them in the high-risk category described in the literature. Their subsequent successful occupational reintegration following individualised multimodal neurorehabilitation is therefore a clinically noteworthy departure from the expected trajectory.
The vocational reorientation of P2, from spray painter to distillery proprietor, raises a question not directly addressed in the existing RTW literature: whether novel vocational self-employment constitutes a categorically different form of recovery from returning to a prior occupation, and whether conventional RTW metrics capture its significance adequately. Brandt et al. (14) reported that most employees with PPCS returned to work but only a minority worked under similar conditions to pre-injury, with employees and managers alike struggling to assess workload accurately. P2’s case suggests that for some patients with PPCS, vocational reorientation toward a different occupation better matched to the post-injury functional state may represent a more sustainable and ultimately more successful outcome than forced return to an occupation whose physical and visual demands may no longer be compatible with the residual deficit profile.
Multimodal neurorehabilitation in chronic PPCS
The evidence base for multimodal neurorehabilitation in chronic PPCS beyond twelve months post-injury is limited but encouraging. Ross et al. (7) reported significant pre-post improvements in both subjective symptom scales and objective measures of trail making, processing speed, reaction time, and visual acuity in a retrospective chart review of patients with PPCS at a mean of approximately two years post-injury, using an intensive five-day multimodal outpatient program. The authors concluded that late-stage PPCS patients may have substantive benefits from a patient-centred, diagnostic- and problem-focused neurorehabilitation approach, and specifically hypothesised that neuroplasticity and sensory entrainment created by rigorous structured neurorehabilitation are efficacious even when patients have clinically plateaued. (7) The present two cases are consistent with this hypothesis, with both patients demonstrating objective neurophysiological improvement and meaningful functional reintegration despite presentations exceeding twelve months post-injury.
The multi-domain objective deficit profiles of both patients, spanning autonomic dysregulation, oculomotor and saccadic circuit impairment, postural instability, and cervicogenic pathology, are consistent with the distributed neurophysiological disruption that characterises PPCS7 and explain why unimodal approaches had not produced functional recovery in either patient prior to referral.
The pathway of care described by Corwin et al. (13) emphasises that visual and vestibular rehabilitation in mTBI should be driven by individual assessment findings and delivered through coordinated multi-modal programs rather than through single-modality protocols, a principle reflected throughout both treatment courses described here.
Saccadometry as a biomarker
Saccadometric findings in both patients were consistent with published characterisations of mTBI-related oculomotor impairment. Heitger et al. (8) demonstrated that latency distribution measurement discriminates between concussed patients and healthy controls, and that saccadometric abnormalities persist well beyond symptomatic resolution in a proportion of PPCS patients. The present cases extend this observation by documenting saccadometric improvement following targeted multimodal rehabilitation, a finding with implications for the use of saccadometry not only as a diagnostic biomarker but also as a treatment response measure. Corwin et al. (9) demonstrated correlations between saccade performance and corpus callosum white matter diffusivity, Stroop performance, and symptom burden, providing a neuroanatomical substrate for the oculomotor deficits measured at baseline in both patients.
The persistence of some saccadometric abnormality at treatment completion in both patients, most notably trajectory scatter, is consistent with the known difficulty of fully normalising frontal-cerebellar circuit timing in established PPCS,7 and is interpreted as reflecting the structural rather than purely functional nature of the underlying circuit impairment.
Oculomotor rehabilitation
P1 and P2’s presenting convergence insufficiency is consistent with the 20.4% prevalence of CI reported by Nordfalk et al. (18) in adults with PPCS and the 23–42% rates reported in military mTBI populations. (19) The CONCUSS clinical trial demonstrated measurable neuroplastic changes in the frontal eye fields, supplemental eye fields, parietal eye fields, cerebellar vermis, and visual cortex following office-based vergence and accommodative rehabilitation for concussion-related CI, (20) consistent with the plasticity of the vergence oculomotor system in the PPCS population and supporting the rationale for targeted vergence rehabilitation as incorporated in the treatment program.
Rhythmic entrainment and timing-based rehabilitation
The entrainment therapy component of both treatment programs, synchronised audiovisual hand clapping with the 54 Hz, is consistent in principle with the Interactive Metronome paradigm, which operates at the same 54-beat-per-minute frequency. Nelson et al. (27) reported in a randomised controlled pilot trial that Interactive Metronome therapy added to standard rehabilitation care for soldiers with persisting cognitive complaints following blast-related TBI produced significant improvements in attention, immediate memory, and delayed memory, with effect sizes in the medium-to-large range and indicators of neuroplastic change accounting for large proportions of the variance in neuropsychological outcomes. The cognitive gains observed in both P1 and P2 across the treatment period, including the cognitive capacity that enabled P2 to undertake online vocational retraining, are consistent with the cognitive rehabilitation mechanism proposed by Nelson et al. (27)
Vestibular rehabilitation and rotational therapy
Vestibular stimulation through the Orbital multi-axis rotational chair provided the primary peripheral vestibular rehabilitation component of both programs. The sagittal roll plane, described as an atypical movement not reproducible in activities of daily living, is consistent with the novel vestibular stimulation paradigms discussed by Sadeghi et al, (18) in the context of unidirectional rotational rebalancing of vestibular asymmetry. Multi-axis rotational therapy has been incorporated as a component of intensive multimodal PPCS programs in the published literature, (7) and audio biofeedback augmentation of vestibular rehabilitation therapy has been shown to produce larger improvements than standard vestibular rehabilitation alone in patients with chronic mTBI and persistent imbalance, with significant effects on both subjective symptom severity and objective sensory organisation testing composite scores. (39) It is the author’s opinion that full body multi axis targeted vestibular stimulation is a driver of enhanced homeostasis. (40, 41, 42, 43)
Cervicogenic management
Cervicogenic pathology was identified and managed in both patients through spinal adjustments targeting documented segmental dysfunction. Nusholtz et al. (15) reported substantive improvement in post-concussive dizziness, headache, and related symptoms following chiropractic management of craniocervical junction dysfunction in patients with PPCS of at least six weeks duration. Bini et al. (16) confirmed in a systematic review and meta-analysis that spinal manipulative therapy produces significant short-term reductions in cervicogenic headache frequency and intensity. The cervicogenic components of both patients’ presentations, headache and restricted range of motion, are likely to have contributed to their overall symptom burden and are appropriately included as targets within the multimodal framework.
Scientific rationale for conclusions
The neurophysiological improvements documented across both cases, and the functional and occupational outcomes that followed, are most parsimoniously explained by neuroplastic reorganisation of the sensory-cognitive-motor networks disrupted by the original mTBI, facilitated by the individualised multimodal rehabilitation program. Ross et al. (7) specifically hypothesised that neuroplasticity and sensory entrainment created by rigorous, diagnostic- and problem-focused structured neurorehabilitation are the mechanisms of efficacy in chronic PPCS, a hypothesis consistent with the findings of the present two cases.
The saccadometric improvements in both patients are consistent with progressive rehabilitation of the frontal-cerebellar circuits mediating response inhibition and spatial remapping. (8, 9) The persistence of some trajectory scatter at treatment completion in both patients is expected given the structural rather than purely functional nature of mTBI-related white matter disruption, and is consistent with the known ceiling of neuroplastic recovery in established PPCS.
The convergence deficit improvement is consistent with the neuroplastic changes in the vergence oculomotor network documented by Alvarez et al.²0 following targeted vergence rehabilitation, supporting a rehabilitation-driven rather than spontaneous mechanism for this component of recovery.
The occupational outcomes of both patients, full return to skilled trade employment for P1 and new vocational self-employment for P2, most likely reflect the aggregate functional recovery across all treated domains rather than improvement in any single domain, consistent with the distributed multidomain nature of the initial neurophysiological deficit profiles. The prior failure of both patients to achieve RTW through standard management argues against spontaneous recovery as the primary explanation for the occupational outcomes.
Conclusions
Primary take-away lessons
These two cases demonstrate that working-age adults with persisting post-concussive symptoms ex- tending beyond twelve months, a population for whom standard management has proven insufficient and whose prognosis for recovery is generally considered poor, can achieve clinically meaningful neurophysiological improvement and meaningful occupational reintegration following individualised, assessment-driven, multimodal neurorehabilitation.
The serial objective neurophysiological data from quantitative pupillometry, saccadometry, and force plate posturography provide documented evidence of measurable change across the treatment period, and the occupational outcomes demonstrate that rehabilitation impact extends to the domains of greatest practical significance for working-age patients.
The contrast between P2’s prior inability to work and his subsequent ability to establish and staff a new commercial enterprise illustrates that in some cases of chronic PPCS the most meaningful vocational outcome is not a return to the prior occupation but an adaptive reorientation that better fits the post-recovery functional state, a nuance not well captured by standard return-to-work metrics.
The cases collectively support the clinical case for a comprehensive, objective assessment-guided, multimodal approach in chronic PPCS, and underscore the importance of treating occupational reintegration, in whatever form it takes, as a primary outcome measure rather than a secondary observation.
Note:
Written informed consent from both patients for the publication of these case reports and the accompanying images is held by the author.
Also by this author
- Richardson D. Two case reports, M46 & M58yo, of long-term stroke recovery using a sensory motor reintegration approach. Asia-Pac Chiropr J. 2026;6.3. www.apcj.net/papers-issue-6-3/#RichardsonStrokeRecovery
- Richardson, D. A functional neurological disorder case series utilising a sensory motor integration model including Chiropractic and vestibular stimulation, Asia-Paci Chiropr J. 2025;5(3). Available at: https://www.apcj.net/papers-issue-5-3/#RichardsonFNeurox4
References
- Greco T, Glenn TC, Hovda DA, Prins ML. Ketogenic diet decreases oxidative stress and improves mitochondrial respiratory complex activity. J Cereb Blood Flow Metab. 2016;36(9):1603–1613. DOI 10.1177/0271678X15610584.
- McDougall A, Bayley M, Munce SE. The ketogenic diet as a treatment for traumatic brain injury: a scoping review. Brain Injury. 2018;32(4):416–422. DOI 10.1080/02699052.2018.1429025.
- Norden DM, Muccigrosso MM, Godbout JP. Microglial priming and enhanced reactivity to secondary insult in aging, and traumatic CNS injury, and neurodegenerative disease. Neuropharmacology. 2015;96(Pt A):29–41. DOI 10.1016/j.neuropharm.2014.10.028. PMID 25445485.
- Dewan MC, Rattani A, Gupta S, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. 2018;130(4):1080–1097. DOI 10.3171/2017.10.JNS17352.
- Polinder S, Cnossen MC, Real RGL, et al. A multidimensional approach to post-concussion symptoms in mild traumatic brain injury. Front Neurol. 2018;9:1113. DOI 10.3389/fneur.2018.01113.
- Dornonville de la Cour FL, Rasmussen MA, Foged EM, Jensen LS, Schow T. Vocational rehabilitation in mild traumatic brain injury: supporting return to work and daily life functioning. Front Neurol. 2019;10:103. DOI 10.3389/fneur.2019.00103.
- Ross EA, Hines RB, Hoffmann M, Jay K, Antonucci MM. Multi-modal neurorehabilitation for persisting post-concussion symptoms. Neurotrauma Rep. 2023;4(1):297–306. DOI 10.1089/neur.2022.0081.
- Heitger MH, Anderson TJ, Jones RD, et al. Saccadometry: the possible application of latency distribution measurement for monitoring concussion. Br J Sports Med. 2004;38(4):489–491. DOI 10.1136/bjsm.2003.009332.
- Corwin DJ, Wiebe DJ, Zonfrillo MR, et al. Antisaccadic eye movements are correlated with corpus callosum white matter mean diffusivity, Stroop performance, and symptom burden in mild traumatic brain injury and concussion. Front Neurol. 2015;6:271. DOI 10.3389/fneur.2015.00271.
- McDonald M, Holdsworth S, Danesh-Meyer H. Eye movements in mild traumatic brain injury: ocular biomarkers. J Eye Mov Res. 2022;15(2):4.
- Al-Husseini A, Gard A, Fransson PA, et al. Long-term postural control in elite athletes following mild traumatic brain injury. Front Neurol. 2022;13:906594. DOI 10.3389/fneur.2022.906594.
- Guskiewicz KM. Postural stability assessment following concussion: one piece of the puzzle. Clin J Sport Med. 2001;11(3):182–9.
- Xiang L, Bansal S, Wu AY, Roberts TL. Pathway of care for visual and vestibular rehabilitation after mild traumatic brain injury: a critical review. Brain Injury. 2022;36(8):911–920. DOI 10.1080/02699052.2022.2105399.
- Conradsen I, Bang-Hansen VE, Sørensen AN, Rytter HM. Return to work in persons with persistent postconcussion symptoms: a survey study examining the perspectives of employees and managers. Brain Injury. 2024;38(11):908–917. DOI 10.1080/02699052.2024.2361620.
- Nusholtz LA, Lim PA, Menezes AH, Burroughs CM. Chiropractic management of the craniocervical junction in post-concussion syndrome: a case series. J Contemp Chiropr. 2021;4:33–41.
- Bini P, Hohenschurz-Schmidt D, Masullo V, et al. The effectiveness of manual and exercise therapy on headache intensity and frequency among patients with cervicogenic headache: a systematic review and meta-analysis. Chiropr Man Therap. 2022;30:49. DOI 10.1186/s12998-022-00459-9.
- Hershaw JN, Barry DM, Ettenhofer ML. Increased risk for age-related impairment in visual attention associated with mild traumatic brain injury: evidence from saccadic response times. PLoS ONE. 2017;12(2):e0171752. DOI 10.1371/journal.pone.0171752.
- Nordfalk KF, Rasmussen MA, Foged EM, Schow T. Convergence insufficiency in patients with post-concussion syndrome is accompanied by a higher symptom load: a cross-sectional study. Brain Inj. 2024;38:1–7. DOI 10.1080/02699052.2024.2334355.
- Scheiman MM, Talasan H, Mitchell GL, Alvarez TL. Objective assessment of vergence after treatment of concussion-related convergence insufficiency: a pilot study. Optom Vis Sci. 2017;94(1):74–88. DOI 10.1097/OPX.0000000000000936.
- Alvarez TL, Vicci VR, Bhoot N, et al. Functional activity changes after vergence and accommodative rehabilitation of concussion-related convergence insufficiency: CONCUSS clinical trial fMRI results. Front Neurol. 2025;16. PMC12583001.
- Silverberg ND, Iverson GL; ACRM Brain Injury Special Interest Group Mild TBI Task Force. The American Congress of Rehabilitation Medicine diagnostic criteria for mild traumatic brain injury. Arch Phys Med Rehabil. 2023;104(8):1343–1355. DOI 10.1016/j.apmr.2023.03.036.
- Mahfuz MM, Schubert MC, Figtree WVC, Todd CJ, Migliaccio AA. Human vestibulo-ocular reflex adaptation training: time beats quantity. J Assoc Res Otolaryngol. 2018;19(6):729–739. DOI 10.1007/s10162-018-00689-w.
- Migliaccio AA, Schubert MC. Unilateral adaptation of the human angular vestibulo-ocular reflex. J Assoc Res Otolaryngol. 2013;14(1):29–36. DOI 10.1007/s10162-012-0359-7.
- Schubert MC, Migliaccio AA. New advances regarding adaptation of the vestibulo-ocular reflex. J Neurophysiol. 2019;122(2):644–658. DOI 10.1152/jn.00729.2018.
- Todd CJ, Hübner PP, Hübner P, Schubert MC, Migliaccio AA. StableEyes - a portable vestibular rehabilitation device. IEEE Trans Neural Syst Rehabil Eng. 2018;26(6):1223–1232. DOI 10.1109/TNSRE.2018.2834964.
- MacDougall HG, McGarvie LA, Halmagyi GM, Curthoys IS, Weber KP. Application of the video head impulse test to detect vertical semicircular canal dysfunction. Otol Neurotol. 2013;34(6):974–9. DOI 10.1097/MAO.0b013e31828d676d.
- Nelson LA, Macdonald M, Stall C, Pazdan R. Effects of interactive metronome therapy on cognitive functioning after blast-related brain injury: a randomized controlled pilot trial. Neuropsychology. 2013;27(6):666–679. DOI 10.1037/a0034117.
- Zaccaro A, Piarulli A, Laurino M, et al. How breath-control can change your life: a systematic review on psycho-physiological correlates of slow breathing. Front Hum Neurosci. 2018;12:353. DOI 10.3389/fnhum.2018.00353.
- O’Brien B, He R, Khuu SK. Establishing the operating conditions of ‘Ocula AI’ in capturing the pupil light reflex. medRxiv. Preprint posted March 3, 2025. DOI 10.1101/2025.03.03.25323271.
- McGrath LB, Eaton J, Abecassis IJ, Maxin A, Kelly C, Chesnut RM, Levitt MR. Mobile smartphone-based digital pupillometry curves in the diagnosis of traumatic brain injury. Front Neurosci. 2022;16:893711. DOI 10.3389/fnins.2022.893711.
- Hall CD, Herdman SJ, Whitney SL, et al. Vestibular rehabilitation for peripheral vestibular hypofunction: an evidence-based clinical practice guideline. J Neurol Phys Ther. 2016;40(2):124–55. DOI 10.1097/NPT.0000000000000120.
- Stöhr M, Petruch F. Somatosensory evoked potentials following stimulation of the trigeminal nerve in man. J Neurol. 1979;220(2):95–98. DOI 10.1007/BF00313949.
- Leandri M, Favale E. Diagnostic relevance of trigeminal evoked potentials following infraorbital nerve stimulation. J Neurosurg. 1991;75(2):244–250. DOI 10.3171/jns.1991.75.2.0244.
- Gagnier JJ, Kienle G, Altman DG, et al. The CARE guidelines: consensus-based clinical case reporting guideline development. J Med Case Rep. 2013;7:223. DOI 10.1186/1752-1947-7-223.
- Silverberg ND, Panenka WJ, Iverson GL. Work productivity loss after mild traumatic brain injury. Arch Phys Med Rehabil. 2018;99(2):250–256. DOI 10.1016/j.apmr.2017.07.006.
- Terry DP, Iverson GL, Panenka W, Colantonio A, Silverberg ND. Workplace and non-workplace mild traumatic brain injuries in an outpatient clinic sample: a case-control study. PLoS One. 2018;13(6):e0198128. DOI 10.1371/journal.pone.0198128.
- de Koning ME, Scheenen ME, van der Horn HJ, et al. Prediction of work resumption and sustainability up to 1 year after mild traumatic brain injury. Neurology. 2017;89(14):1542–8. DOI 10.1212/WNL.0000000000004604.
- Sadeghi NG, Sabetazad B, Rassaian N, Sadeghi SG. Rebalancing the vestibular system by unidirectional rotations in patients with chronic vestibular dysfunction. Front Neurol. 2019;9:1196. DOI 10.3389/fneur.2018.01196..
- Campbell KR, Peterka RJ, Fino PC, et al. The effects of augmenting traditional rehabilitation with audio biofeedback in people with persistent imbalance following mild traumatic brain injury. Front Neurol. 2022;13:926691. DOI 10.3389/fneur.2022.926691.
- Richardson, D. (2026) 'Two case reports, M46 & M58yo, of long-term stroke recovery using a sensory motor reintegration approach', Asia-Pacific Chiropractic Journal, 6(3). Available at: www.apcj.net/papers-issue-6-3/#RichardsonStrokeRecovery .
- Richardson, D. (2024) 'Functional neurological disorder and chiropractic: two case reports’, Chiropractic Journal of Australia, 51(1), pp. 1–25.
- Richardson, D. (2022) 'A novel treatment for Persistent Postural Perceptual Dizziness (3PD): a case report', Chiropractic Journal of Australia, 49(1), pp. 1–24.
- Richardson, D. (2025) 'A functional neurological disorder case series utilising a sensory motor integration model including Chiropractic and vestibular stimulation', Asia-Pacific Chiropractic Journal, 5(3). Available at: https://www.apcj.net/papers-issue-5-3/#RichardsonFNeurox4
Timelines
Patient 1:
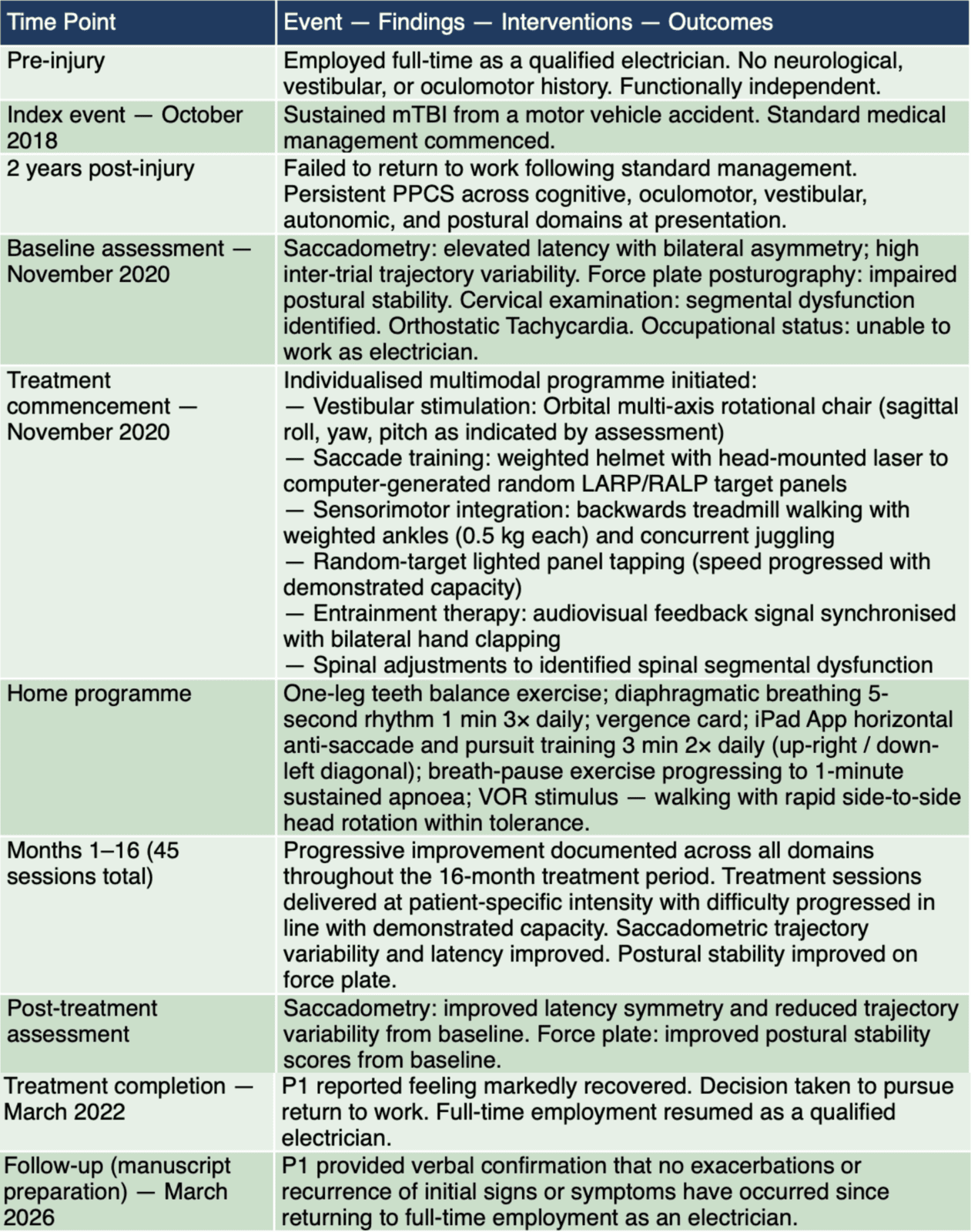
Patient 2:
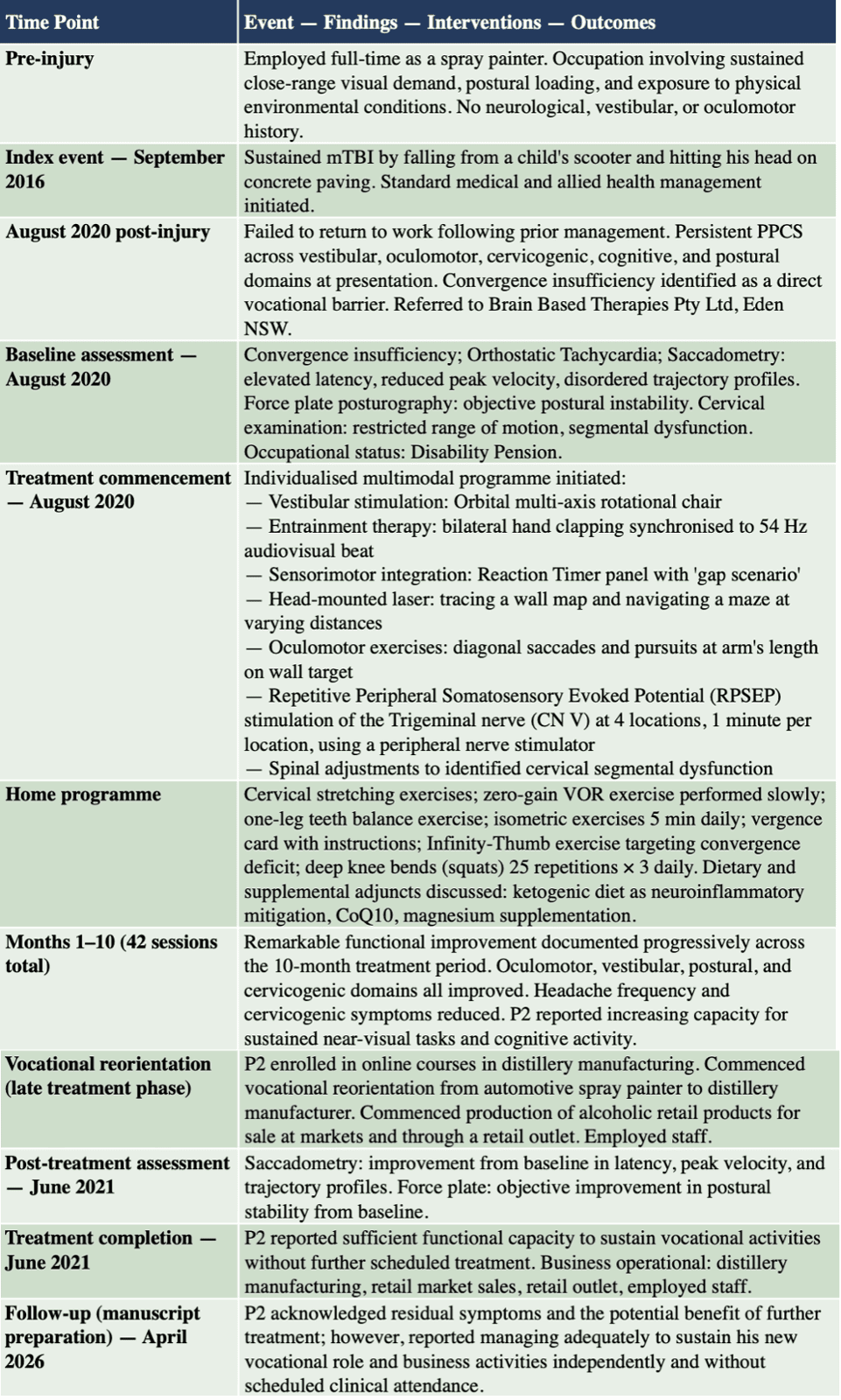
Selected abstracts

Each issue we select some abstracts that interest us from the many scientific symposia Chiropractors hold globally
Today we bring you a case report from the Australian Gonstead Clinical Studies group, an eclectic abstract from an AK scientific meeting, and an abstract of a case report from the Proceedings of an SOT scientific symposium.
We do not provide a PDF of these presentations but link you to the original source document of each.
AU: Albert Apalvik, B.App.Sc (Clin) B.Chiro.Sc GCS Diplomate. Private practice, Oslo, Norway.
The purpose of this study is to highlight the correlation between spinal subluxations and dizziness of benign origin. There are several possible causes of dizziness and underlying pathology should always be ruled out first. That said, the potential neurological disturbance from a subluxated vertebrae as a primary cause should not be overlooked.
This case study reveals the benefits that a patient may experience when a subluxation is identified and corrected in a specific manner.
Indexing terms: Dizziness; Chiropractic; Subluxation; Nervous system; Vestibular system; Gonstead.
Originally published as:
Cite: Apalvik A. Chiropractic management of dizziness. International Journal of practicing Chiropractors. Case Studies - Gonstead. 2023. Dizziness Vestibular System. At Dizziness Vestibular System-Apalvik A
Introduction
Dizziness is a complex and potentially debilitating symptom affecting up to 30% of the global population. Annually it accounts for over three million emergency department visits. (1) It can manifest across all age groups, though it is notably more prevalent among adults aged 65 and above due to an increased likelihood of underlying health conditions. The condition is two to three times more common in females. (2) The word dizziness itself is a vague and
broad description of a condition, which is perceived and experienced very differently between individuals.
Dizziness is commonly characterised by feelings of unsteadiness, spinning, disorientation, or perceived movement. (3) Characteristics, intensity, duration and frequency also vary greatly among patients and may guide a practitioner to a likely cause and diagnosis. There are numerous aetiologies that can result in dizziness including vestibular, neurological, cardiovascular, and musculoskeletal disorders. Among these, the role of musculoskeletal issues, particularly those involving the cervical spine, is of particular interest to chiropractic care.
Common causes are problems or conditions that affects the ears such as Meniere´s disease and labyrinthitis, eye conditions, heart issues, stress, dehydration, low blood sugar levels, chemical or hormonal imbalances, infections or neurological disorders. (4)
Treating a patient with dizziness normally involves identifying and addressing its underlying cause, which can be varied and sometimes multifactorial. Given the complexity of the causes, treatments can range greatly. They include: repositioning procedures such as lifestyle changes, the Epley Maneuver, physical therapy, medication and surgery. (5)
Signs and symptoms such as confusion, difficulty speaking or understanding language, sudden severe headache or vomiting without known cause, weakness in extremities are potential red flags that should be referred out for immediate medical examination first. (6) Such possible pathological conditions are beyond the scope of this paper.
The Gonstead chiropractic system, named after its originator Clarence S Gonstead, is a specific, detailed, and practical approach to chiropractic care that meticulously addresses biomechanical dysfunction of the spine and extremities. Examination procedures in the Gonstead method are comprehensive and the objective is to identify potential vertebral subluxations. These are biomechanical dysfunctions due to positional dyskinesia of a functional spinal unit (FSU) predominately in the spine, sacroiliac joints or temporomandibular joint (TMJ), that can create directly or indirectly neurological disturbances. (7) This can have a tremendous effect on neurological function not only at that spinal segment, but also on the entire body as altered afferent input to the central nervous system leads to abnormal somatosensory processing and therefore altered sensorimotor integration and output. (8)
The Gonstead chiropractic adjustment aims to correct these subluxations with specificity and accuracy to restore optimal spinal function and remove any associated nerve interference. The protocol may also incorporate guidance on lifestyle modifications to support overall well-being and prevent recurrence.
This case study examines a patient's journey through dizziness, managed via the Gonstead Chiropractic system. It aims to investigate the effectiveness of this method in addressing dizziness, of a benign aetiology believed to be due to spinal subluxations. By doing so, this study seeks to expand the relatively limited body of research on the role of specific Chiropractic techniques, like the Gonstead method, in managing common yet often mismanaged symptoms such as dizziness.
Case history
An 81-year-old female presented with continuous dizziness and neck stiffness. The dizziness was described as a constant feeling of perceived movement and mild spinning. She reported feeling unsteady at times, but there were no tendencies of falling or fainting. Getting up or moving aggravated the symptoms. Lying down reduced the symptoms. The symptoms started suddenly two weeks prior after painting her ceiling. She had no headache, but a sensation of pressure in her head was present intermittently. No obvious spinal pain or referred neurological symptoms in extremities were present. Examination by a medical doctor and MRI of the head and cervical spine the previous week revealed no abnormalities and she was instructed to rest and give it time to pass. As this did not change her symptoms, she decided to seek a chiropractic evaluation for an opinion and alternative treatment for her ailments.
Previously, nine months earlier, she had attended our clinic for pain in the lumbosacral area that resolved after adjustments at sacrum (S2), left sacroiliac joint (SIJ) and L2 over the course of three weeks. She did not drink coffee or consume any forms of drugs. No history of trauma, infection or use of medication was reported. She had finished treatment for anal cancer 5 year prior with no signs of recurrence. Otherwise, her medical history was unremarkable.
Clinical findings
Observation of the patient showed an elderly lady in general good health and appearance. She did show signs of head pressure discomfort and was trying not to move to avoid aggravating the symptoms of dizziness.
Cranial nerve screen testing was normal. Romberg’s test showed general instability withmtendency to sway forward to the left.
Chiropractic examination revealed:
• Instrumentation (spinal skin temperature differential): reading detected at the C7 andT9 levels
• Static palpation: Point tenderness and edema noted at C7 and T9 spinous processes
• Hypertonic right thoracic erector spinae muscle from T6-T9 and right superior trapezius muscle
• Motion palpation: Restricted flexion and extension of C7 on T1 and T9 on T10
Radiographic examination
Full spine, weight bearing radiographic images using Gonstead acquisition protocols were taken of the patient. Please refer to x-ray images at the end of this paper. The listings derived from the full spine radiographs were:
• Left ASIN ilium, S2 posterior, L3 PRI-M, T9 PLI-T and C7 PLI-La.
• Degenerated intervertebral discs were noted between C3 and C7
Chiropractic diagnosis
Following full Gonstead Chiropractic history, examination and spinographic findings, the initial diagnoses made for the above cases were:
• T9 PLI-T and C7 PLI-La.
Treatment outcome
On the first visit, both T9 and C7 were adjusted. T9 with the patient prone on the hi-lo table taking a pisiform contact on the right transverse/lamina junction. C7 taking a index finger contact on the right spinous/lamina junction with the patient seated in cervical chair. Only minor movements and cavitations were noted during these adjustments. The patient returned a week later, where she reported an increase of dizziness and neck stiffness the day after the
first adjustments, before rapid improvement in symptoms over the following days. Only minor dizziness during sudden movements was now present.
Gonstead examination indicated a subluxation at T9 was still present and therefore this segment was adjusted again.
The last visit was one week later where she reported feeling normal with no further signs of dizziness. T9 was adjusted with minimal force and depth on this visit, and she was instructed to contact the clinic if the symptoms returned. The primary symptoms a year later have not returned. She did report over a recent phone conversation in relation to this paper that she intermittently gets mild signs of dizziness over a short duration. She attributes this to her use of glasses, and being age appropriate. These tendencies are so mild she has not felt the need to at this point get examined by a Chiropractor or her medical doctor.
Discussion
Dizziness is a commonly reported condition and can manifest in various presentations. As Chiropractors our aim is not to primarily diagnose or name a condition, but rather try to identify the true cause behind it. Although for the purpose of this case study, it is also valuable to understand when dizziness is not a benign complaint that may require a referral for medical management or co-management. The chiropractor must understand the four primary types of dizziness: vertigo, pre-syncope, disequilibrium, and nonspecific dizziness. (9)
Understanding these four categories of dizziness provides a framework to evaluate, diagnose, and manage patients presenting with this common, yet multifaceted symptom. It also aids in determining the potential cause of the dizziness, which will ultimately guide the choice of treatment strategy. (10)
Neurologically, the vertebral subluxation complex theory suggests that spinal misalignment or structural dyskinesia of a functional spinal unit (FSU) can lead to direct or indirect aberrant neurological function. When this occurs, various symptoms may develop, including dizziness. a biomechanical injury and inflammatory responses to the FSU, as seen in subluxations, given proximity to nerve roots, dorsal root ganglion (DRG), spinal cord and associated neurons, is
very likely to affect these delicate tissues. These are all located inside the dural sheath and are extremely sensitive to pressure from biomechanical dysfunction, chemical irritants or ischemic impacts. (11) This is especially true in the intervertebral foramen (IVF) where dorsal and ventral roots, DRG, spinal arteries and veins, the dural sheath and CSF pass through. In addition, associated disc protrusions, disc herniations and degeneration combined with arthritic changes to the facet joints can lead to further narrowing of the IVF and probable nerve root compression. (12)
The central nervous system (CNS), including the brain and spinal cord, is the primary system for coordinating all body activities. As such, any subluxations may disrupt or distort the messages traveling along these neural pathways, potentially leading to a range of symptoms.
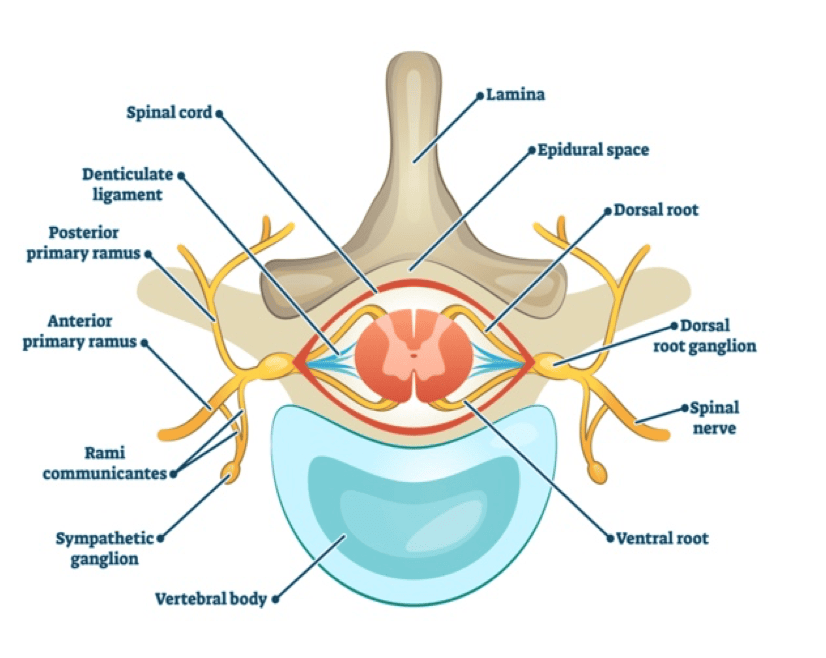
In this case study, even subluxations outside the cervical area could have created neurological disturbances affecting the vestibular nuclei located in the brainstem or its connections, leading to sensations of unsteadiness.
Biomechanically, the spine functions as a coherent unit with interdependence between its various components. For example, a lumbar or thoracic subluxation may cause compensatorychanges higher up in the spine. (13) This can affect balance and proprioception and its associated complex responses in the brain, potentially leading to sensations of dizziness.
Spinal subluxations can contribute to the sensation of dizziness through multiple intricate neurophysiological pathways.
One crucial concept is that the vertebral column houses the spinal cord, a significant component of the central nervous system (CNS). This communication highway facilitates the transfer of sensory and motor information between the brain and the rest of the body. Any interference in this communication, such as that potentially caused by spinal subluxations, can lead to a range of symptoms, including dizziness. (14)
Direct or indirect mechanical pressure or chemical irritation on the spinal nerves or the spinal cord due to subluxations can cause neurological disturbances. This interference can disrupt the normal transmission of nerve impulses to the vestibular renters in the brain responsible for maintaining balance and spatial orientation. (15) Altered or distorted information received by these centres can result in a sensation of dizziness.
Proprioception, the body's sense of position and movement in space, is also a crucial player. Particularly in the cervical spine, proprioceptive information significantly contributes to our sense of balance. Spinal subluxations can disrupt accurate proprioceptive input to the brain, creating a sensory mismatch with other systems maintaining balance, like the vestibular system and vision, leading to dizziness. (16)
Vertebrobasilar insufficiency, a condition characterised by reduced blood flow through the vertebral arteries due to mechanical compression, often associated with cervical subluxations or as compensations for subluxations in other spinal regions, can also cause dizziness. The vertebral arteries supply the posterior brain, including the cerebellum and brainstem, crucial areas for maintaining balance. (17)
Likely most relevant for this case study and many cases of dizziness caused by spinal subluxations is the Vestibular system.
Our sense of balance and spatial orientation is controlled by an intricate sensory system known as the vestibular system, which resides in a part of the inner ear called the vestibular labyrinth. The vestibular system is composed of the following elements (18):
Semicircular Canals: These are three tubes that are oriented nearly perpendicular to each other. Each canal is sensitive to a unique type of movement - upward and downward nodding, side-to-side shaking, or tilting to the right or left. The fluid-filled canals respond to these specific movements, as the fluid shifts within them accordingly Otolith Organs: These consist of two structures capable of detecting linear movement, gravitational pull, and tilting actions. Comprising the utricle and saccule, the otolith organs are composed of calcium carbonate crystals. While the utricle is sensitive to horizontal motion, the saccule picks up on vertical movement.
The information from these vestibular organs is conveyed to the brainstem nuclei via the vestibular nerve. This information is then dispatched to other components of the central nervous system, including the cerebellum and cerebral cortex, where it is utilised to coordinate movement. The proper functioning of the system requires both vestibular organs, located on either side of the head, to transmit balanced signals to the brain. For the human body to maintain balance the vestibular system functions by sensing the orientation of our bodies relative to gravity. In addition, it also provides sensory input regarding equilibrium and body movement. The cerebellum can utilise this information together with sensory input from eyes as well as proprioceptive input from the musculoskeletal to coordinate balance. If thecerebellum detects insufficient balance it will communicate with appropriate muscle groups to restore balance. (19)
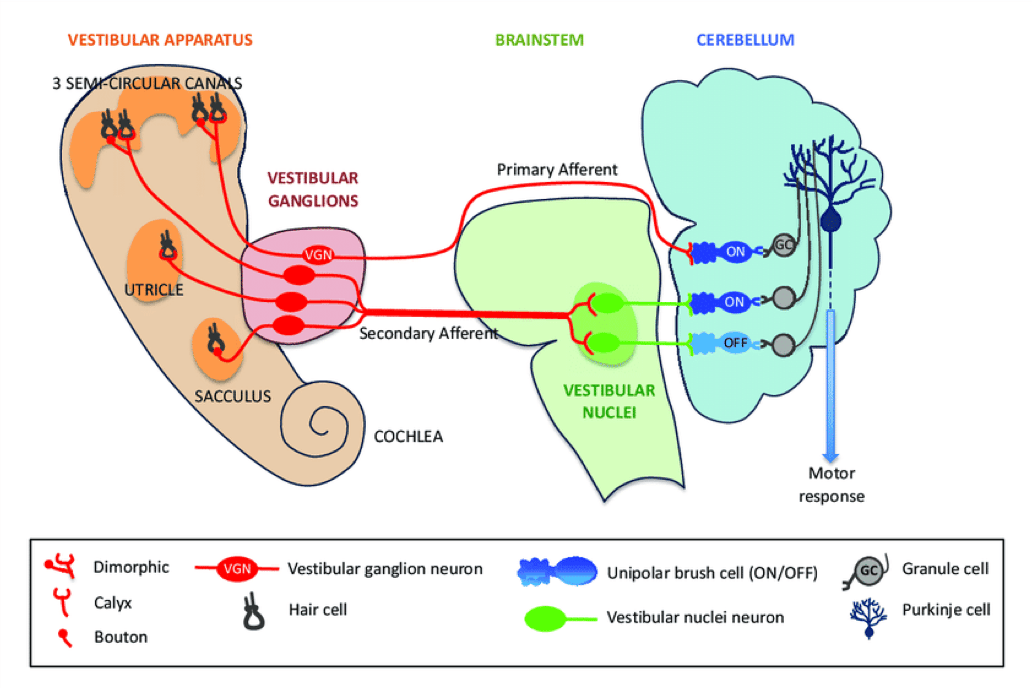
The patient in this case study underwent a detailed evaluation under the Gonstead chiropractic system, which identified specific subluxations. After receiving precise Gonstead chiropractic adjustments aimed at correcting these subluxations, the patient reported a significant reduction and eventually full remission of her dizziness.
This highlights the importance of holistic care in Chiropractic practice and suggests that subluxations in areas even outside the cervical spine can also contribute to symptoms of dizziness. Such findings expand our understanding of the interplay between spinal integrity and patient health, emphasising the potential of Gonstead chiropractic in managing dizziness. In summary, spinal subluxations can induce dizziness through direct and indirect neurological pathways and by altering cerebral blood flow. This intricate neurophysiology underscores the potential role of Chiropractic interventions in managing dizziness.
Conclusion
This case study focuses on a patient who presented with dizziness of benign origin and responded favourably to the Gonstead Chiropractic analysis and adjustments. This is despite the absence of any upper cervical subluxation or dysfunction, which is the area of the spine one might first suspect a subluxation to be present for this condition.
The positive outcome observed highlights the potential influence of spinal subluxations and the associated neural interferences triggering this symptom, underscoring the intricate neurological and biomechanical interconnections within the human body.
Gonstead and many other Gonstead practitioners with him have noted the common correlation between upper cervical subluxations and dizziness. Some cases have also demonstrated involvement of the TMJ. (20) They have also reported that subluxations below the cervical spine, even to the level of the pelvic region, could result in such symptoms.
Hence going back to the philosophy of the founding father of Chiropractic DD Palmer: he made it clear to accept the subluxation where you find it! Gonstead was also very clear to point this out, and also how important it was to leave it alone once the signs of subluxations were reduced or absent.
When underlying pathology is ruled out, Chiropractic examination for potential nerve interference arising from a spinal subluxation should be considered in cases of dizziness. When we study the anatomy, biomechanics and neurology of the spine, it makes logical sense that nerve interference from a subluxation has the capacity to create signs and symptoms of dizziness.
Note: Image references are given in the original publication.
1. https://www.ncbi.nlm.nih.gov/books/NBK470308/
2. https://pubmed.ncbi.nlm.nih.gov/27638063/
3. https://www.mayoclinic.org/diseases-conditions/dizziness/symptoms-causes/
4. https://www.healthdirect.gov.au/dizziness
5. https://www.betterhealth.vic.gov.au/health/conditionsandtreatments/dizziness-and-vertigo#treatment-of-dizziness
6. https://www.healthdirect.gov.au/dizziness
7. Gonstead Chiroractic Society Australia. Gonstead Chiropractic, Essential package. iBooks, Apple. 2020. p.219
8. Gonstead Chiroractic Society Australia. Gonstead Chiropractic, Essential package. iBooks, Apple. 2020. p. 280
9. BM Reilly, Clinical Methods: the history, physical and laboratory examinations, 3e, Chapter 212 Dizziness, Pub; Butterworths 1990.
10. https://www.ncbi.nlm.nih.gov/books/NBK325/
11. Gonstead Chiroractic Society Australia. Gonstead Chiropractic, Essential package. iBooks, Apple. 2020. p.252
12. Gonstead Chiroractic Society Australia. Gonstead Chiropractic, Essential package. iBooks, Apple. 2020. p. 255
13. Gonstead Chiroractic Society Australia. Gonstead Chiropractic, Essential package. iBooks, Apple. 2020. Book 5, p. 174, Book 6, p. 290.
14. Kulkarni, V., Chandy, M. J., & Babu, K. S. (2001). Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India, 49(4), 355
15. Brandt, T., & Bronstein, A. M. (2001). Cervical vertigo. Journal of Neurology, Neurosurgery & Psychiatry, 71(1), 8-12
16. L'Heureux-Lebeau, B., Godbout, A., Berbiche, D., & Saliba, I. (2014). Evaluation of paraclinical tests in the diagnosis of cervicogenic dizziness. Otolaryngology–Head and Neck Surgery, 151(1), 159-165
17. Lee, H., Sohn, S. I., Cho, Y. W., Lee, S. R., Ahn, B. H., Park, B. R., & Baloh, R. W. (2006). Cervical vertigo: correlation with radiographic findings. Acta Oto-
laryngologica, 126(10), 1038-44 .
18. Britannica, The Editors of Encyclopaedia. "vestibular system". Encyclopedia Britannica,
19. https://premierneurologycenter.com/blog/the-vestibular-system-what-it-is-and-how-it- affects-balance/
20. Cox, John W. In the footsteps of Dr.G; Our lives with C.S. Gonstead. 2003. p 221. 20 Sep. 2019, https://www.britannica.com/science/vestibular-system.
AU: William E. Sisson Jr., MA, DC. Private practice of Chiropractic, Wilmington, NC. e: bill@billsissonhealthcare.com
Abstract There may be a connection between the Qi (life force energy) and the Injury Recall Technique (IRT) developed by Dr Walter Schmitt, Jr, DC, DIBAK, DACBN. This same connection may apply to muscles that fail the autogenic inhibition (spindle cell approximation) test. It may also be relevant in cases where a Beginning or End (B&E) point of the acupuncture channels that originate or terminate on the face is used more than once during a patient visit.
Objective Develop a process based on Manual Muscle Testing (MMT) that includes this energy factor when clearing the confusion from the Central Nervous System (CNS) which may cause erroneous findings with MMT.
Method The new methodology utilises the IRT manoeuvre in combination with Therapy Localisation (TL) to the appropriate acupuncture Alarm (MU) point to address the energetic component in the procedures mentioned above. It has been used during the last one- and one-half years in an Applied Kinesiology (AK) practice to clear interference patterns from the CNS prior to treating patients’ clinical complaints.
Result Most of the patients tested demonstrated a need to have this energetic element cleared when eliminating reflexes arising from traumas and other stress-related events.
Conclusion An energetic imbalance appears to be a result of the many stresses that lead to confusion in the CNS. Use of the IRT manoeuvre in combination with the patient’s TL to the Mu Point of the appropriate acupuncture channel can eliminate this component.
Indexing terms IRT; Alarm/Mu point; LQM; Set Point; Switching; Autogenic Inhibition.
Originally published as:
Cite: Sisson WE. IRT and B&E The Qi Connection. In: Experimental Observations of Members of the ICAK Volume 1, 2023-2024 Seventy-Fourth Collection of the Proceedings of the Annual Meeting. International College of Applied Kinesiology. pp. 53-5. Available here.
Introduction
Dr Wally Schmitt adapted the Injury Recall Technique (IRT) from the work of Dr Gordon Bronston, a podiatrist in Michigan. Bronston had learned his technique from its developer, Robert Croty, DPM and had used it while treating Schmitt for an ankle injury.
IRT uses a light ankle toggle or micro flexion of the occiput on the atlas, if trauma occurs above the shoulders, to eliminate the flexor-withdrawal type of neurological reflex associated with trauma.
Other challenges can be used to uncover hidden trauma reflexes. These include having the patient direct their eyes toward the site of the injury, turning the head and lateral spinal flexion.
Schmitt named this more in-depth assessment Beyond IRT. (Schmitt Seminar Beyond IRT, Wilmington, NC, 1996)
The brain can also store the memories associated with trauma. Dr. Schmitt treated these with the Location, Quality and Memory (LQM) technique. In LQM the traumatic reflex is neutralised by stimulating the appropriate B&E point when the patient recalls an aspect of the traumatic event muscle to weaken.
B&E points are utilized for other clearing procedures as well. These include the B&E technique (Walther, Applied Kinesiology Synopsis, 2d. ED., 2000, pp. 277-278), the Nociceptive Stimulation Blocking (NSB) technique (Quintessential Applications,
The Neurological Rationale for a Comprehensive Clinical Protocol Using Applied Kinesiology Techniques 2005 AKSP), the Cover One Eye Cerebellar Challenge (Synchronising the CNS, QA Home Study webinar, July 2020) the REM Challenge (QA Webinars – To Sleep or not to Sleep – part 1, July 2019), the
Emotional Recall technique and the Set Point technique that Schmitt developed with Michael Lebowitz, DC (1989 Selected Papers of the ICAK, pp. 25-32).
Materials and Methods
All evaluative testing was done with MMT. The procedure involved tapping the relevant B&E point while the patient therapy localised the appropriate MU point.
Discussion
About three years ago I observed that if a B&E point might be used more than once during a patient visit. I found that an indicator muscle would be inhibited when the patient therapy localised the Mu point for either the channel whose B&E point was used more than once or for its paired yin channel and a IRT challenge was done . Applying the IRT corrective manoeuvre while the patient maintained the TL would negate the positive challenge. I routinely perform this
procedure now as part of my IRT clearing procedure.
This energetic connection may also exist in the case of a hypertonic muscle. Schmitt taught that IRT could help reset muscles that are over facilitated. Such a muscle would be hypertonic to MMT and would not be inhibited by spindle cell compression. According to Schmitt’s procedure stimulating the muscle’s origin and insertion (O&I) and then performing IRT would reset the muscle to its normal resting state. Several of the patients I treated in this fashion returned with the same hypertonicity on a follow up visit.
I found that TL to the MU point of the acupuncture channel that ran through the muscle would recreate the muscle’s hypertonicity even after the O&I/IRT correction. I hypothesised that there might be an energetic component to the muscle’s hypertonicity that was not addressed by the O&I/IRT correction alone.
The procedure I developed as a result of my hypothesis is to first determine if spindle cell compression inhibits a muscle. If this test fails, treat the muscle as Dr. Schmitt taught. Next have the patient therapy localise the MU point for the acupuncture channel running through themuscle and re-test the muscle. For muscles that accommodate more than one acupuncture channel several MU points may have to be tested. If the muscle fails to respond to spindle cell
compression, the patient continues to TL the MU point while the IRT manoeuvre is again performed.
Recheck with both TL to the origin/insertion and to the MU point with the IRT challenge to determine that the muscle has been reset to normal. The procedure can be performed in the reverse order of that just described. When I have cleared the muscle using the MU point first the number of times I then have to retreat using O&I is less than vice versa.
Results
TL to the MU point of the indicated acupuncture channel together with the IRT manoeuvre in addition to the O&I/IRT method described by Schmitt seems to restore a hypertonic muscle to a normal response pattern and prevents recidivism. In addition, an IRT challenge to the MU point of any B&E acupuncture channel used more than once during a patient visit that inhibits an indicator muscle seems to indicate a hidden IRT pattern that should be corrected.
Conclusion
When the CNS cannot compensate for the accumulation of stresses to which it is subjected it creates confusion in the system. It may also affect the body’s QI. This effect can manifest through hypertonic muscles and through other procedures that involve the use of B&E points. It can be detected with MMT when TL to the MU point for the acupuncture channel involved combined with an IRT challenge causes the inhibition of an indicator muscle . The imbalance can be corrected by using the IRT manoeuvre while maintaining the TL to the MU point.
More research is needed to confirm these findings.
References
5. Schmitt, Walter H. and Lebowitz, Michael: Hypothalamic Set Point Technique, Selected Papers of the ICAK, 1989 pp. 25-32
AU 1: Ibis Melissa Roman Guzman, DC. A graduate from Life University, with a Master’s in Environmental Risk Management and Assessment and a Bachelor’s in Biology with a concentration in Microbiology. Currently, she is a professor at the Universidad Central del Caribe and a chiropractor at the Hospital Regional de Castañer,
AU 2: Jake Halverson, DC.
Originally published as:
Cite: Guzman IMR, Halverson J. Focal nodular hyperplasia of the liver incidentally identified in a chiropractic patient with rib pain, a case report. In:
Objective
To describe an adult male with focal nodular hyperplasia (FNH) of the liver mimicking right lower rib pain.
Clinical Features
A 42-year-old male presented with right lower rib pain extending from the midsternal to the midaxillary line. The pain was sharp, aching, and radiating. He had a history of liver laceration after blunt abdominal trauma 34 years prior.
Interventions/outcomes
Murphy’s sign was positive, and there was reduced and painful right lateral thoracic bending. Palpation of the anterior right lower ribs elicited epigastric pain. An Activator instrument-assisted adjustment was performed on rib 8, which did not relieve the pain.
The working diagnosis was intercostal neuralgia. The patient was referred for a sonographic examination of the gall bladder to discard acute cholecystitis. The sonogram revealed an incidental large hypervascular liver mass. Multiphase contrast abdominal computed tomography was performed to further characterise the lesion, demonstrating a mildly hyperattenuating, and moderately enhancing 8.8 cm mass in the left lobe of the liver, with hypoattenuating central scar, consistent with FNH.
Conclusion
Remote trauma may predispose patients to developing painful visceral lesions that mimic musculoskeletal pain. Diagnostic imaging plays a crucial role in securing the diagnosis and directing appropriate management.
A philosophical moment
Thoughts from Professor Tirthankar Ghosh, Dean, Sri Sri University